Young Jin Yoo, Deok-Gie Kim, Eun-Ki Min, Seung Hyuk Yim, Mun Chae Choi, Hwa-Hee Koh, Minyu Kang, Jae Geun Lee, Myoung Soo Kim, Dong Jin Joo
{"title":"移植前治疗性血浆交换次数增加abo血型不相容活体肝移植患者肝细胞癌复发风险","authors":"Young Jin Yoo, Deok-Gie Kim, Eun-Ki Min, Seung Hyuk Yim, Mun Chae Choi, Hwa-Hee Koh, Minyu Kang, Jae Geun Lee, Myoung Soo Kim, Dong Jin Joo","doi":"10.3389/ti.2025.14304","DOIUrl":null,"url":null,"abstract":"<p><p>Previous studies have reported comparable oncologic outcome between ABO-incompatible (ABOi) living donor liver transplantation (LDLT) and ABO-compatible (ABOc) LDLT in patients with hepatocellular carcinoma (HCC). We aimed to analyze the relationship between number of therapeutic plasma exchanges (TPE) before LDLT and HCC outcomes in ABOi LDLT. In this single-center retrospective study, 428 adult LDLT recipients with HCC were categorized into three groups according to ABO incompatibility and the number of pretransplant TPE: ABOc (n = 323), ABOi/TPE ≤5 (n = 75), and ABOi/TPE ≥6 (n = 30). The RFS and HCC recurrence rates were compared. Three groups showed similar characteristics in most demographics, pretransplant tumor markers and pathologies. The median initial isoagglutinin (IA) titer was 1:64 (range negative-1:512) in ABOi/TPE ≤5 group and 1:512 (range 1:128-1:4,096) in ABOi/TPE ≥6 group. Five-year RFS was significantly lower (75.7% vs. 72.7% vs. 50.0%, P = 0.005) and HCC recurrence was significantly higher in the ABOi/TPE ≥6 group than in the other groups(16.4% vs. 17.0% vs. 39.4%, P = 0.014). In multivariable Cox regression analysis, ABOi/TPE ≥6 was an independent risk factor for RFS (aHR 1.99, 95% CI:1.02-3.86, P = 0.042) and HCC recurrence (aHR 2.42, 95% CI:1.05-5.57, P = 0.037). More than six pretransplant TPE sessions may increase the risk of HCC recurrence after ABOi LDLT. Reducing TPE sessions to fewer than six should be considered while maintaining immunological stability through IA titer control.</p>","PeriodicalId":23343,"journal":{"name":"Transplant International","volume":"38 ","pages":"14304"},"PeriodicalIF":3.0000,"publicationDate":"2025-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380628/pdf/","citationCount":"0","resultStr":"{\"title\":\"Number of Pretransplant Therapeutic Plasma Exchange Sessions Increase the Recurrence Risk of Hepatocellular Carcinoma in ABO-Incompatible Living Donor Liver Transplantation.\",\"authors\":\"Young Jin Yoo, Deok-Gie Kim, Eun-Ki Min, Seung Hyuk Yim, Mun Chae Choi, Hwa-Hee Koh, Minyu Kang, Jae Geun Lee, Myoung Soo Kim, Dong Jin Joo\",\"doi\":\"10.3389/ti.2025.14304\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Previous studies have reported comparable oncologic outcome between ABO-incompatible (ABOi) living donor liver transplantation (LDLT) and ABO-compatible (ABOc) LDLT in patients with hepatocellular carcinoma (HCC). We aimed to analyze the relationship between number of therapeutic plasma exchanges (TPE) before LDLT and HCC outcomes in ABOi LDLT. In this single-center retrospective study, 428 adult LDLT recipients with HCC were categorized into three groups according to ABO incompatibility and the number of pretransplant TPE: ABOc (n = 323), ABOi/TPE ≤5 (n = 75), and ABOi/TPE ≥6 (n = 30). The RFS and HCC recurrence rates were compared. Three groups showed similar characteristics in most demographics, pretransplant tumor markers and pathologies. The median initial isoagglutinin (IA) titer was 1:64 (range negative-1:512) in ABOi/TPE ≤5 group and 1:512 (range 1:128-1:4,096) in ABOi/TPE ≥6 group. Five-year RFS was significantly lower (75.7% vs. 72.7% vs. 50.0%, P = 0.005) and HCC recurrence was significantly higher in the ABOi/TPE ≥6 group than in the other groups(16.4% vs. 17.0% vs. 39.4%, P = 0.014). In multivariable Cox regression analysis, ABOi/TPE ≥6 was an independent risk factor for RFS (aHR 1.99, 95% CI:1.02-3.86, P = 0.042) and HCC recurrence (aHR 2.42, 95% CI:1.05-5.57, P = 0.037). More than six pretransplant TPE sessions may increase the risk of HCC recurrence after ABOi LDLT. Reducing TPE sessions to fewer than six should be considered while maintaining immunological stability through IA titer control.</p>\",\"PeriodicalId\":23343,\"journal\":{\"name\":\"Transplant International\",\"volume\":\"38 \",\"pages\":\"14304\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/ti.2025.14304\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/ti.2025.14304","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
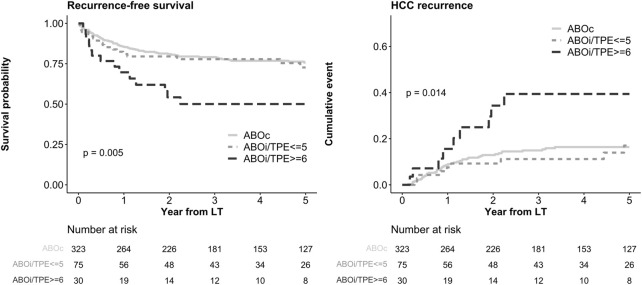
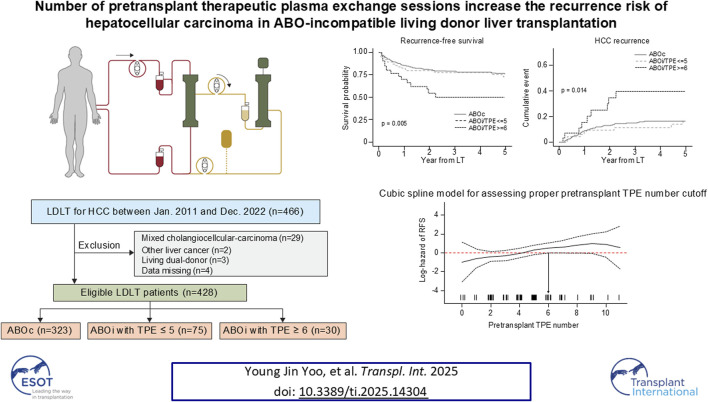
先前的研究报道了abo -不相容(ABOi)活体供肝移植(LDLT)和abo -相容(ABOc) LDLT在肝细胞癌(HCC)患者中的肿瘤预后相当。我们的目的是分析LDLT前治疗性血浆交换(TPE)次数与ABOi LDLT患者HCC结局之间的关系。在这项单中心回顾性研究中,428名成年HCC LDLT受者根据ABO不相容性和移植前TPE数量分为三组:ABOc (n = 323)、ABOi/TPE≤5 (n = 75)和ABOi/TPE≥6 (n = 30)。比较RFS和HCC复发率。三组在大多数人口统计学、移植前肿瘤标志物和病理上表现出相似的特征。ABOi/TPE≤5组的初始异凝集素(IA)滴度中位数为1:64(范围为负1:12 12),ABOi/TPE≥6组的初始异凝集素滴度中位数为1:12 12(范围为1:128 ~ 1:4 096)。ABOi/TPE≥6组的5年RFS显著低于其他组(75.7% vs. 72.7% vs. 50.0%, P = 0.005), HCC复发率显著高于其他组(16.4% vs. 17.0% vs. 39.4%, P = 0.014)。在多变量Cox回归分析中,ABOi/TPE≥6是RFS (aHR 1.99, 95% CI:1.02 ~ 3.86, P = 0.042)和HCC复发(aHR 2.42, 95% CI:1.05 ~ 5.57, P = 0.037)的独立危险因素。移植前TPE超过6次可能会增加ABOi LDLT术后HCC复发的风险。应考虑将TPE减少到6次以下,同时通过控制IA滴度来保持免疫稳定性。
Number of Pretransplant Therapeutic Plasma Exchange Sessions Increase the Recurrence Risk of Hepatocellular Carcinoma in ABO-Incompatible Living Donor Liver Transplantation.
Previous studies have reported comparable oncologic outcome between ABO-incompatible (ABOi) living donor liver transplantation (LDLT) and ABO-compatible (ABOc) LDLT in patients with hepatocellular carcinoma (HCC). We aimed to analyze the relationship between number of therapeutic plasma exchanges (TPE) before LDLT and HCC outcomes in ABOi LDLT. In this single-center retrospective study, 428 adult LDLT recipients with HCC were categorized into three groups according to ABO incompatibility and the number of pretransplant TPE: ABOc (n = 323), ABOi/TPE ≤5 (n = 75), and ABOi/TPE ≥6 (n = 30). The RFS and HCC recurrence rates were compared. Three groups showed similar characteristics in most demographics, pretransplant tumor markers and pathologies. The median initial isoagglutinin (IA) titer was 1:64 (range negative-1:512) in ABOi/TPE ≤5 group and 1:512 (range 1:128-1:4,096) in ABOi/TPE ≥6 group. Five-year RFS was significantly lower (75.7% vs. 72.7% vs. 50.0%, P = 0.005) and HCC recurrence was significantly higher in the ABOi/TPE ≥6 group than in the other groups(16.4% vs. 17.0% vs. 39.4%, P = 0.014). In multivariable Cox regression analysis, ABOi/TPE ≥6 was an independent risk factor for RFS (aHR 1.99, 95% CI:1.02-3.86, P = 0.042) and HCC recurrence (aHR 2.42, 95% CI:1.05-5.57, P = 0.037). More than six pretransplant TPE sessions may increase the risk of HCC recurrence after ABOi LDLT. Reducing TPE sessions to fewer than six should be considered while maintaining immunological stability through IA titer control.
期刊介绍:
The aim of the journal is to serve as a forum for the exchange of scientific information in the form of original and high quality papers in the field of transplantation. Clinical and experimental studies, as well as editorials, letters to the editors, and, occasionally, reviews on the biology, physiology, and immunology of transplantation of tissues and organs, are published. Publishing time for the latter is approximately six months, provided major revisions are not needed. The journal is published in yearly volumes, each volume containing twelve issues. Papers submitted to the journal are subject to peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


