{"title":"西太平洋区域结核病预防治疗的进展和挑战:对七个结核病高负担国家的情况分析。","authors":"Kyung Hyun Oh, Alvin Kuo Jing Teo, Manami Yanagawa, Avinash Kanchar, Dennis Falzon, Cecily Miller, Youngeun Choi, Gyeong In Lee, Fukushi Morishita, Kalpeshsinh Rahevar, Huong Thi Giang Tran, Rajendra Prasad Hubraj Yadav","doi":"10.1186/s41182-025-00805-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tuberculosis preventive treatment (TPT) can avert progression from infection to disease, yet scale-up across the World Health Organization Western Pacific Region is patchy. To guide acceleration, we assessed progress, challenges and responses in seven high-burden countries-Cambodia, China, Lao People's Democratic Republic (PDR), Mongolia, Papua New Guinea, the Philippines and Viet Nam-drawing on 2015-2023 programme data, structured questionnaires, follow-up interviews and a regional validation workshop.</p><p><strong>Main body: </strong>Six of the seven countries have issued national TPT guidelines and five now offer shorter rifapentine- or rifampicin-based regimens. The number of people started on TPT rose sharply in most settings, driven by household contacts aged ≥ 5 years in Cambodia, Mongolia and the Philippines and by people living with HIV in Lao PDR and Papua New Guinea. However, coverage of children under five and other high-risk groups remains low. Cascade analysis revealed major attrition between screening and TPT initiation. Key obstacles, viewed through a socio-ecological lens, include: individual complacency, fear of adverse events and limited provider confidence; stigma and consent barriers in migrant households; intermittent staff training, medicine stock-outs and weak digital tools; long journeys to health facilities; and policy-practice gaps such as the absence of child-friendly formulations and non-notification of tuberculosis infection. Countries and partners endorsed a tiered package combining patient-centred counselling, mobile reminders, shorter paediatric regimens, stigma-reduction campaigns and remote e-consent. Health systems will reinforce staff training, digital supply-chain and adherence tools, while decentralised one-stop outreach and community health-workers extend coverage. A multisector task force will fast-track paediatric fixed-dose registration, make infection notifiable and absorb preventive treatment costs into national budgets and insurance schemes.</p><p><strong>Conclusions: </strong>The introduction of shorter regimens and rising enrolment confirm that rapid gains are achievable, yet wide disparities persist across age groups, risk categories and care-cascade stages. Implementing the agreed client, community, institutional and policy interventions-backed by integrated governance and sustainable domestic funding-can convert TPT from a promising guideline into a routine, life-saving component of primary health care throughout the Western Pacific Region.</p>","PeriodicalId":23311,"journal":{"name":"Tropical Medicine and Health","volume":"53 1","pages":"122"},"PeriodicalIF":3.5000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12403340/pdf/","citationCount":"0","resultStr":"{\"title\":\"Progress and challenges in tuberculosis preventive treatment in the Western Pacific Region: a situational analysis of seven high tuberculosis burden countries.\",\"authors\":\"Kyung Hyun Oh, Alvin Kuo Jing Teo, Manami Yanagawa, Avinash Kanchar, Dennis Falzon, Cecily Miller, Youngeun Choi, Gyeong In Lee, Fukushi Morishita, Kalpeshsinh Rahevar, Huong Thi Giang Tran, Rajendra Prasad Hubraj Yadav\",\"doi\":\"10.1186/s41182-025-00805-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Tuberculosis preventive treatment (TPT) can avert progression from infection to disease, yet scale-up across the World Health Organization Western Pacific Region is patchy. To guide acceleration, we assessed progress, challenges and responses in seven high-burden countries-Cambodia, China, Lao People's Democratic Republic (PDR), Mongolia, Papua New Guinea, the Philippines and Viet Nam-drawing on 2015-2023 programme data, structured questionnaires, follow-up interviews and a regional validation workshop.</p><p><strong>Main body: </strong>Six of the seven countries have issued national TPT guidelines and five now offer shorter rifapentine- or rifampicin-based regimens. The number of people started on TPT rose sharply in most settings, driven by household contacts aged ≥ 5 years in Cambodia, Mongolia and the Philippines and by people living with HIV in Lao PDR and Papua New Guinea. However, coverage of children under five and other high-risk groups remains low. Cascade analysis revealed major attrition between screening and TPT initiation. Key obstacles, viewed through a socio-ecological lens, include: individual complacency, fear of adverse events and limited provider confidence; stigma and consent barriers in migrant households; intermittent staff training, medicine stock-outs and weak digital tools; long journeys to health facilities; and policy-practice gaps such as the absence of child-friendly formulations and non-notification of tuberculosis infection. Countries and partners endorsed a tiered package combining patient-centred counselling, mobile reminders, shorter paediatric regimens, stigma-reduction campaigns and remote e-consent. Health systems will reinforce staff training, digital supply-chain and adherence tools, while decentralised one-stop outreach and community health-workers extend coverage. A multisector task force will fast-track paediatric fixed-dose registration, make infection notifiable and absorb preventive treatment costs into national budgets and insurance schemes.</p><p><strong>Conclusions: </strong>The introduction of shorter regimens and rising enrolment confirm that rapid gains are achievable, yet wide disparities persist across age groups, risk categories and care-cascade stages. Implementing the agreed client, community, institutional and policy interventions-backed by integrated governance and sustainable domestic funding-can convert TPT from a promising guideline into a routine, life-saving component of primary health care throughout the Western Pacific Region.</p>\",\"PeriodicalId\":23311,\"journal\":{\"name\":\"Tropical Medicine and Health\",\"volume\":\"53 1\",\"pages\":\"122\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2025-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12403340/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tropical Medicine and Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41182-025-00805-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"TROPICAL MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tropical Medicine and Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41182-025-00805-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"TROPICAL MEDICINE","Score":null,"Total":0}
Progress and challenges in tuberculosis preventive treatment in the Western Pacific Region: a situational analysis of seven high tuberculosis burden countries.
Background: Tuberculosis preventive treatment (TPT) can avert progression from infection to disease, yet scale-up across the World Health Organization Western Pacific Region is patchy. To guide acceleration, we assessed progress, challenges and responses in seven high-burden countries-Cambodia, China, Lao People's Democratic Republic (PDR), Mongolia, Papua New Guinea, the Philippines and Viet Nam-drawing on 2015-2023 programme data, structured questionnaires, follow-up interviews and a regional validation workshop.
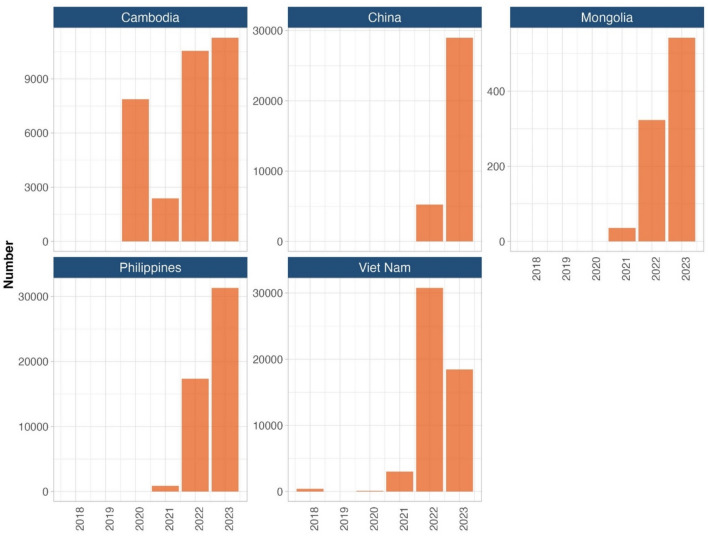
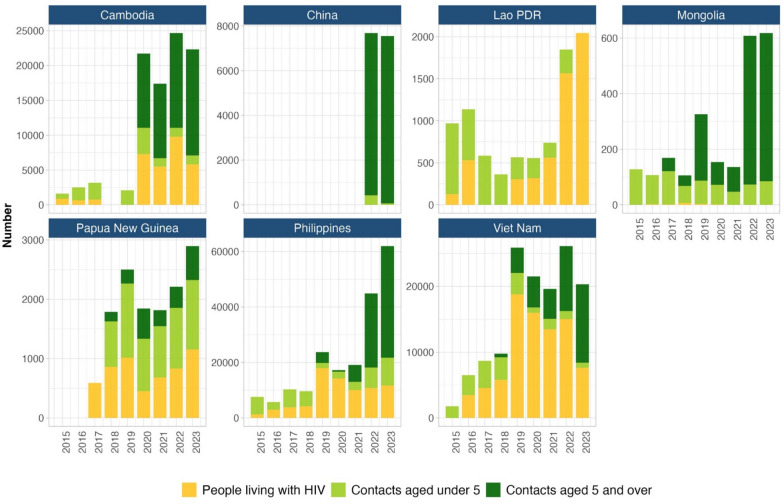
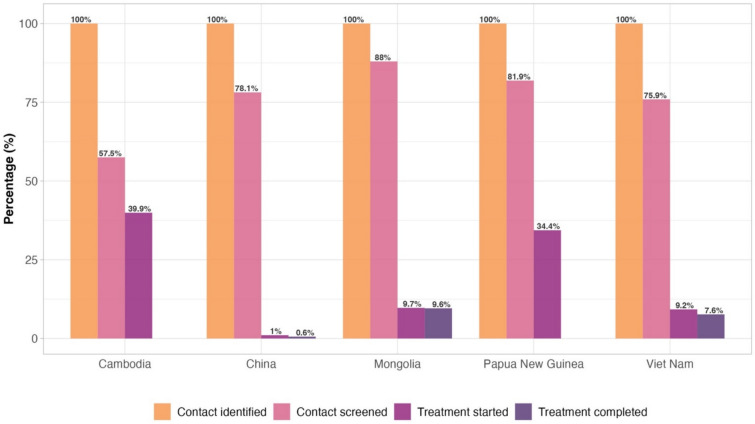
Main body: Six of the seven countries have issued national TPT guidelines and five now offer shorter rifapentine- or rifampicin-based regimens. The number of people started on TPT rose sharply in most settings, driven by household contacts aged ≥ 5 years in Cambodia, Mongolia and the Philippines and by people living with HIV in Lao PDR and Papua New Guinea. However, coverage of children under five and other high-risk groups remains low. Cascade analysis revealed major attrition between screening and TPT initiation. Key obstacles, viewed through a socio-ecological lens, include: individual complacency, fear of adverse events and limited provider confidence; stigma and consent barriers in migrant households; intermittent staff training, medicine stock-outs and weak digital tools; long journeys to health facilities; and policy-practice gaps such as the absence of child-friendly formulations and non-notification of tuberculosis infection. Countries and partners endorsed a tiered package combining patient-centred counselling, mobile reminders, shorter paediatric regimens, stigma-reduction campaigns and remote e-consent. Health systems will reinforce staff training, digital supply-chain and adherence tools, while decentralised one-stop outreach and community health-workers extend coverage. A multisector task force will fast-track paediatric fixed-dose registration, make infection notifiable and absorb preventive treatment costs into national budgets and insurance schemes.
Conclusions: The introduction of shorter regimens and rising enrolment confirm that rapid gains are achievable, yet wide disparities persist across age groups, risk categories and care-cascade stages. Implementing the agreed client, community, institutional and policy interventions-backed by integrated governance and sustainable domestic funding-can convert TPT from a promising guideline into a routine, life-saving component of primary health care throughout the Western Pacific Region.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


