{"title":"巨大纵隔神经鞘瘤合并1型神经纤维瘤病的外科治疗1例。","authors":"Shin-Nosuke Watanabe, Daisuke Kimura, Kengo Tani, Takahiro Sasaki, Shuta Kimura, Chisaki Muto, Tsubasa Kato, Masahito Minakawa","doi":"10.70352/scrj.cr.25-0150","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Neurogenic tumors commonly develop in the posterior mediastinum in both pediatric and adult patients. In patients with neurofibromatosis type 1, distinguishing benign schwannomas from malignant peripheral nerve sheath tumors is challenging. In this study, we aimed to present the surgical management of a giant schwannoma that required differentiation from a malignant peripheral nerve sheath tumor.</p><p><strong>Case presentation: </strong>A 15-year-old boy presented with a large right mediastinal mass discovered on chest radiography at high school admission. Subsequent contrast-enhanced CT of the chest showed the development of a large tumor (16.0 × 12.5 × 11.8 cm) occupying approximately two-thirds of the right thoracic cavity, with atelectasis of the lower lobe of the right lung. The patient was histopathologically diagnosed with a benign schwannoma associated with neurofibromatosis type 1 through a thoracoscopic biopsy of the tumor and had received oral selumetinib at 50-70 mg/day for 11 months. Surgical excision was performed because of tumor progression and suspected malignant transformation. Right posterolateral thoracotomy with the opening of the 6th intercostal space was performed by extending the anterior skin incision along the abdominal rectus muscle and separating the 6th costal cartilage and diaphragmatic margin along the chest wall. The tumor was completely removed by resecting numerous adhesions between the tumor and the surrounding tissues and coagulating several nutrient vessels that flowed into the tumor, while resecting the lower lobe of the lung. The postoperative course was uneventful. The pathological examination revealed no malignancy. Subsequent contrast-enhanced CT of the chest revealed no residual tumors.</p><p><strong>Conclusions: </strong>Posterolateral thoracotomy with the separation of the costal cartilage and diaphragmatic margin along the chest wall could achieve safe surgery for a giant mediastinal schwannoma.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377975/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Management of a Giant Mediastinal Schwannoma Associated with Neurofibromatosis Type 1: A Case Report.\",\"authors\":\"Shin-Nosuke Watanabe, Daisuke Kimura, Kengo Tani, Takahiro Sasaki, Shuta Kimura, Chisaki Muto, Tsubasa Kato, Masahito Minakawa\",\"doi\":\"10.70352/scrj.cr.25-0150\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Neurogenic tumors commonly develop in the posterior mediastinum in both pediatric and adult patients. In patients with neurofibromatosis type 1, distinguishing benign schwannomas from malignant peripheral nerve sheath tumors is challenging. In this study, we aimed to present the surgical management of a giant schwannoma that required differentiation from a malignant peripheral nerve sheath tumor.</p><p><strong>Case presentation: </strong>A 15-year-old boy presented with a large right mediastinal mass discovered on chest radiography at high school admission. Subsequent contrast-enhanced CT of the chest showed the development of a large tumor (16.0 × 12.5 × 11.8 cm) occupying approximately two-thirds of the right thoracic cavity, with atelectasis of the lower lobe of the right lung. The patient was histopathologically diagnosed with a benign schwannoma associated with neurofibromatosis type 1 through a thoracoscopic biopsy of the tumor and had received oral selumetinib at 50-70 mg/day for 11 months. Surgical excision was performed because of tumor progression and suspected malignant transformation. Right posterolateral thoracotomy with the opening of the 6th intercostal space was performed by extending the anterior skin incision along the abdominal rectus muscle and separating the 6th costal cartilage and diaphragmatic margin along the chest wall. The tumor was completely removed by resecting numerous adhesions between the tumor and the surrounding tissues and coagulating several nutrient vessels that flowed into the tumor, while resecting the lower lobe of the lung. The postoperative course was uneventful. The pathological examination revealed no malignancy. Subsequent contrast-enhanced CT of the chest revealed no residual tumors.</p><p><strong>Conclusions: </strong>Posterolateral thoracotomy with the separation of the costal cartilage and diaphragmatic margin along the chest wall could achieve safe surgery for a giant mediastinal schwannoma.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377975/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0150\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0150","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/22 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Surgical Management of a Giant Mediastinal Schwannoma Associated with Neurofibromatosis Type 1: A Case Report.
Introduction: Neurogenic tumors commonly develop in the posterior mediastinum in both pediatric and adult patients. In patients with neurofibromatosis type 1, distinguishing benign schwannomas from malignant peripheral nerve sheath tumors is challenging. In this study, we aimed to present the surgical management of a giant schwannoma that required differentiation from a malignant peripheral nerve sheath tumor.
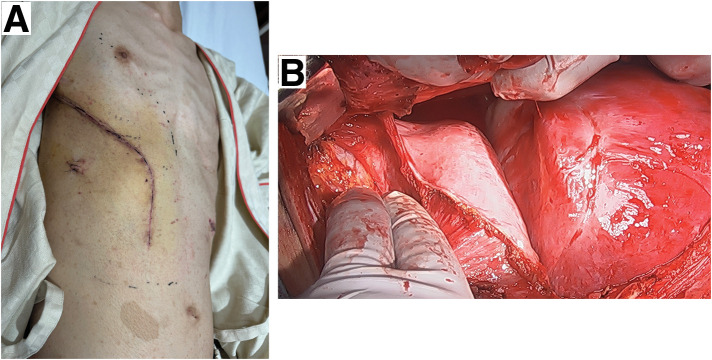
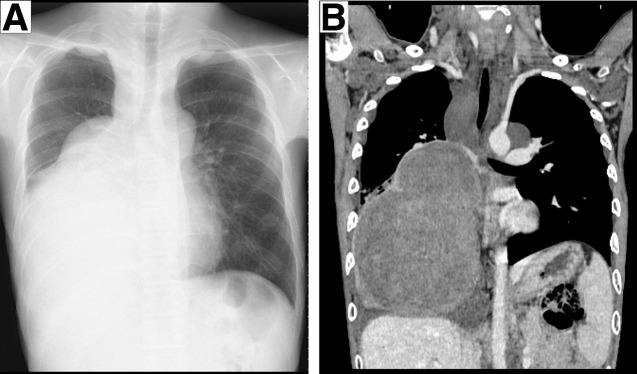
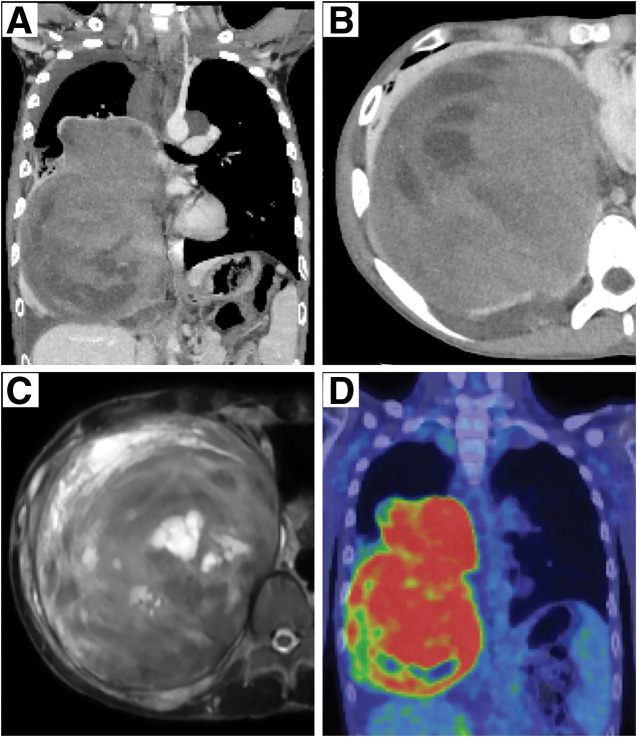
Case presentation: A 15-year-old boy presented with a large right mediastinal mass discovered on chest radiography at high school admission. Subsequent contrast-enhanced CT of the chest showed the development of a large tumor (16.0 × 12.5 × 11.8 cm) occupying approximately two-thirds of the right thoracic cavity, with atelectasis of the lower lobe of the right lung. The patient was histopathologically diagnosed with a benign schwannoma associated with neurofibromatosis type 1 through a thoracoscopic biopsy of the tumor and had received oral selumetinib at 50-70 mg/day for 11 months. Surgical excision was performed because of tumor progression and suspected malignant transformation. Right posterolateral thoracotomy with the opening of the 6th intercostal space was performed by extending the anterior skin incision along the abdominal rectus muscle and separating the 6th costal cartilage and diaphragmatic margin along the chest wall. The tumor was completely removed by resecting numerous adhesions between the tumor and the surrounding tissues and coagulating several nutrient vessels that flowed into the tumor, while resecting the lower lobe of the lung. The postoperative course was uneventful. The pathological examination revealed no malignancy. Subsequent contrast-enhanced CT of the chest revealed no residual tumors.
Conclusions: Posterolateral thoracotomy with the separation of the costal cartilage and diaphragmatic margin along the chest wall could achieve safe surgery for a giant mediastinal schwannoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


