Mohamed F Doheim, Robrecht R M M Knapen, Julie Staals, Wouter J Schonewille, Diederik W J Dippel, Adriaan C G M van Es, Hester F Lingsma, Christiaan van der Leij, Charles B Majoie, Raul G Nogueira, Robert J van Oostenbrugge, Wim H van Zwam
{"title":"直接血管内与桥接治疗大脑中动脉M2段闭塞:MR CLEAN登记研究。","authors":"Mohamed F Doheim, Robrecht R M M Knapen, Julie Staals, Wouter J Schonewille, Diederik W J Dippel, Adriaan C G M van Es, Hester F Lingsma, Christiaan van der Leij, Charles B Majoie, Raul G Nogueira, Robert J van Oostenbrugge, Wim H van Zwam","doi":"10.1161/STROKEAHA.125.051967","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal strategy for managing M2 segment occlusions of the middle cerebral artery, whether with direct endovascular treatment (EVT) or bridging therapy with intravenous thrombolysis (IVT) before EVT, remains unclear. This study aimed to evaluate the effectiveness and safety of both approaches.</p><p><strong>Methods: </strong>Patients with M2 segment occlusions of the middle cerebral artery, treated between March 2014 and December 2018, were identified from the MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands), a prospective, nationwide, multicenter registry of patients with acute ischemic stroke who underwent endovascular treatment during that period. They were divided into 2 groups: those who received IVT followed by EVT, and those who received EVT alone. Primary outcomes included functional outcomes at 90 days, assessed by ordinal logistic regression analysis of modified Rankin Scale (mRS) scores. Secondary outcomes included recanalization rates measured by extended Thrombolysis in Cerebral Infarction scores, dichotomized mRS scores (0-1, 0-2, and 0-3), death at 90 days, and symptomatic intracranial hemorrhage. All analyses were performed using both unadjusted and adjusted multivariable approaches, with adjustment achieved through inverse probability of treatment weighting to account for baseline imbalances, including age, baseline National Institutes of Health Stroke Scale score, prior stroke, history of atrial fibrillation, anticoagulant use, and transfer status.</p><p><strong>Results: </strong>A total of 539 patients with M2 occlusions were included in the analysis: 377 received IVT+EVT and 162 received EVT alone. The median age was significantly lower in the IVT+EVT group compared with the EVT-alone group (71 [61-79] versus 74 [65-81]; <i>P</i>=0.01), whereas the proportion of male patients was similar between groups (55.2% versus 51.9%; <i>P</i>=0.15). At 90 days, inverse probability of treatment weighting analysis showed that IVT+EVT was significantly associated with reduced disability compared with EVT alone (adjusted common odds ratio for mRS score, 1.52 [95% CI, 1.04-2.21]; <i>P</i>=0.03). Dichotomized functional outcomes and mortality were numerically in favor of IVT+EVT, with higher rates of mRS score of 0 to 1 (38.9% versus 29.7%, aOR, 1.40 [95% CI, 0.85-2.30]; <i>P</i>=0.19), mRS score of 0 to 2 (57.8% versus 46.5%; aOR, 1.42 [95% CI, 0.88-2.29]; <i>P</i>=0.15), and mRS score of 0 to 3 (73.2% versus 59.4%, aOR, 1.54 [95% CI, 0.94-2.51]; <i>P</i>=0.09), as well as lower 90-day mortality (17.2% versus 25.8%; aOR, 0.83 [95% CI, 0.47-1.45]; <i>P</i>=0.51). In contrast, recanalization rates and symptomatic intracranial hemorrhage were numerically in favor of EVT alone, but all these differences were not statistically significant (<i>P</i>>0.05).</p><p><strong>Conclusions: </strong>Bridging therapy may yield superior functional outcomes compared with EVT alone for patients with the middle cerebral artery-M2 occlusions.</p>","PeriodicalId":21989,"journal":{"name":"Stroke","volume":" ","pages":"2866-2878"},"PeriodicalIF":8.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447822/pdf/","citationCount":"0","resultStr":"{\"title\":\"Direct Endovascular Versus Bridging Therapy in M2 Segment Occlusion of Middle Cerebral Artery: A MR CLEAN Registry Study.\",\"authors\":\"Mohamed F Doheim, Robrecht R M M Knapen, Julie Staals, Wouter J Schonewille, Diederik W J Dippel, Adriaan C G M van Es, Hester F Lingsma, Christiaan van der Leij, Charles B Majoie, Raul G Nogueira, Robert J van Oostenbrugge, Wim H van Zwam\",\"doi\":\"10.1161/STROKEAHA.125.051967\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The optimal strategy for managing M2 segment occlusions of the middle cerebral artery, whether with direct endovascular treatment (EVT) or bridging therapy with intravenous thrombolysis (IVT) before EVT, remains unclear. This study aimed to evaluate the effectiveness and safety of both approaches.</p><p><strong>Methods: </strong>Patients with M2 segment occlusions of the middle cerebral artery, treated between March 2014 and December 2018, were identified from the MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands), a prospective, nationwide, multicenter registry of patients with acute ischemic stroke who underwent endovascular treatment during that period. They were divided into 2 groups: those who received IVT followed by EVT, and those who received EVT alone. Primary outcomes included functional outcomes at 90 days, assessed by ordinal logistic regression analysis of modified Rankin Scale (mRS) scores. Secondary outcomes included recanalization rates measured by extended Thrombolysis in Cerebral Infarction scores, dichotomized mRS scores (0-1, 0-2, and 0-3), death at 90 days, and symptomatic intracranial hemorrhage. All analyses were performed using both unadjusted and adjusted multivariable approaches, with adjustment achieved through inverse probability of treatment weighting to account for baseline imbalances, including age, baseline National Institutes of Health Stroke Scale score, prior stroke, history of atrial fibrillation, anticoagulant use, and transfer status.</p><p><strong>Results: </strong>A total of 539 patients with M2 occlusions were included in the analysis: 377 received IVT+EVT and 162 received EVT alone. The median age was significantly lower in the IVT+EVT group compared with the EVT-alone group (71 [61-79] versus 74 [65-81]; <i>P</i>=0.01), whereas the proportion of male patients was similar between groups (55.2% versus 51.9%; <i>P</i>=0.15). At 90 days, inverse probability of treatment weighting analysis showed that IVT+EVT was significantly associated with reduced disability compared with EVT alone (adjusted common odds ratio for mRS score, 1.52 [95% CI, 1.04-2.21]; <i>P</i>=0.03). Dichotomized functional outcomes and mortality were numerically in favor of IVT+EVT, with higher rates of mRS score of 0 to 1 (38.9% versus 29.7%, aOR, 1.40 [95% CI, 0.85-2.30]; <i>P</i>=0.19), mRS score of 0 to 2 (57.8% versus 46.5%; aOR, 1.42 [95% CI, 0.88-2.29]; <i>P</i>=0.15), and mRS score of 0 to 3 (73.2% versus 59.4%, aOR, 1.54 [95% CI, 0.94-2.51]; <i>P</i>=0.09), as well as lower 90-day mortality (17.2% versus 25.8%; aOR, 0.83 [95% CI, 0.47-1.45]; <i>P</i>=0.51). In contrast, recanalization rates and symptomatic intracranial hemorrhage were numerically in favor of EVT alone, but all these differences were not statistically significant (<i>P</i>>0.05).</p><p><strong>Conclusions: </strong>Bridging therapy may yield superior functional outcomes compared with EVT alone for patients with the middle cerebral artery-M2 occlusions.</p>\",\"PeriodicalId\":21989,\"journal\":{\"name\":\"Stroke\",\"volume\":\" \",\"pages\":\"2866-2878\"},\"PeriodicalIF\":8.9000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447822/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1161/STROKEAHA.125.051967\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/STROKEAHA.125.051967","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Direct Endovascular Versus Bridging Therapy in M2 Segment Occlusion of Middle Cerebral Artery: A MR CLEAN Registry Study.
Background: The optimal strategy for managing M2 segment occlusions of the middle cerebral artery, whether with direct endovascular treatment (EVT) or bridging therapy with intravenous thrombolysis (IVT) before EVT, remains unclear. This study aimed to evaluate the effectiveness and safety of both approaches.
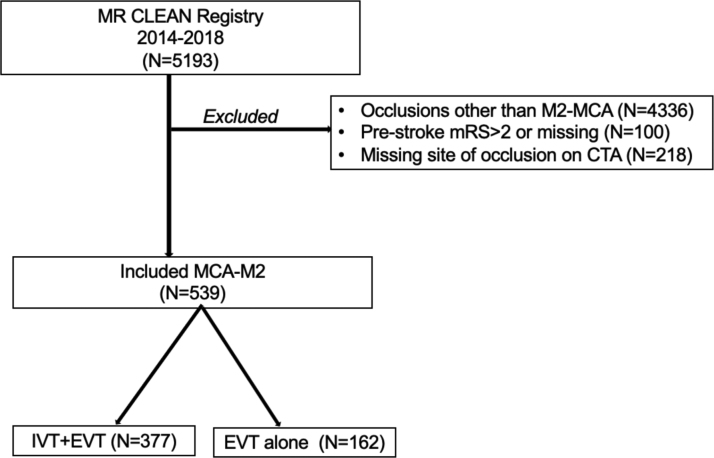
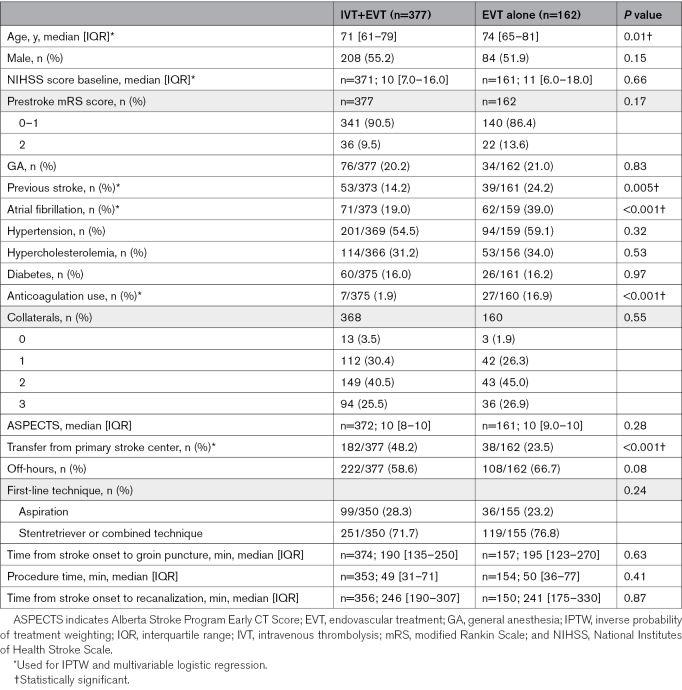
Methods: Patients with M2 segment occlusions of the middle cerebral artery, treated between March 2014 and December 2018, were identified from the MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands), a prospective, nationwide, multicenter registry of patients with acute ischemic stroke who underwent endovascular treatment during that period. They were divided into 2 groups: those who received IVT followed by EVT, and those who received EVT alone. Primary outcomes included functional outcomes at 90 days, assessed by ordinal logistic regression analysis of modified Rankin Scale (mRS) scores. Secondary outcomes included recanalization rates measured by extended Thrombolysis in Cerebral Infarction scores, dichotomized mRS scores (0-1, 0-2, and 0-3), death at 90 days, and symptomatic intracranial hemorrhage. All analyses were performed using both unadjusted and adjusted multivariable approaches, with adjustment achieved through inverse probability of treatment weighting to account for baseline imbalances, including age, baseline National Institutes of Health Stroke Scale score, prior stroke, history of atrial fibrillation, anticoagulant use, and transfer status.
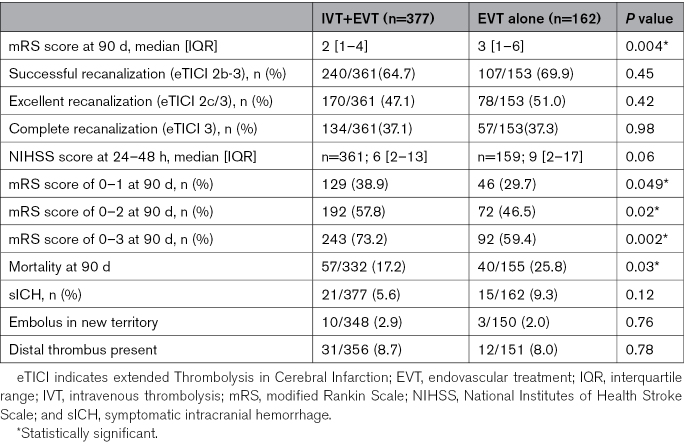
Results: A total of 539 patients with M2 occlusions were included in the analysis: 377 received IVT+EVT and 162 received EVT alone. The median age was significantly lower in the IVT+EVT group compared with the EVT-alone group (71 [61-79] versus 74 [65-81]; P=0.01), whereas the proportion of male patients was similar between groups (55.2% versus 51.9%; P=0.15). At 90 days, inverse probability of treatment weighting analysis showed that IVT+EVT was significantly associated with reduced disability compared with EVT alone (adjusted common odds ratio for mRS score, 1.52 [95% CI, 1.04-2.21]; P=0.03). Dichotomized functional outcomes and mortality were numerically in favor of IVT+EVT, with higher rates of mRS score of 0 to 1 (38.9% versus 29.7%, aOR, 1.40 [95% CI, 0.85-2.30]; P=0.19), mRS score of 0 to 2 (57.8% versus 46.5%; aOR, 1.42 [95% CI, 0.88-2.29]; P=0.15), and mRS score of 0 to 3 (73.2% versus 59.4%, aOR, 1.54 [95% CI, 0.94-2.51]; P=0.09), as well as lower 90-day mortality (17.2% versus 25.8%; aOR, 0.83 [95% CI, 0.47-1.45]; P=0.51). In contrast, recanalization rates and symptomatic intracranial hemorrhage were numerically in favor of EVT alone, but all these differences were not statistically significant (P>0.05).
Conclusions: Bridging therapy may yield superior functional outcomes compared with EVT alone for patients with the middle cerebral artery-M2 occlusions.
期刊介绍:
Stroke is a monthly publication that collates reports of clinical and basic investigation of any aspect of the cerebral circulation and its diseases. The publication covers a wide range of disciplines including anesthesiology, critical care medicine, epidemiology, internal medicine, neurology, neuro-ophthalmology, neuropathology, neuropsychology, neurosurgery, nuclear medicine, nursing, radiology, rehabilitation, speech pathology, vascular physiology, and vascular surgery.
The audience of Stroke includes neurologists, basic scientists, cardiologists, vascular surgeons, internists, interventionalists, neurosurgeons, nurses, and physiatrists.
Stroke is indexed in Biological Abstracts, BIOSIS, CAB Abstracts, Chemical Abstracts, CINAHL, Current Contents, Embase, MEDLINE, and Science Citation Index Expanded.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


