Sophie Holcik, Lamia Hawayi, Naomi Dussah, Nick Barrowman, Nadya Ben Fadel, Bernard Thébaud, Sherri Lynne Katz
{"title":"极度早产伴支气管肺发育不良儿童2岁时严重呼吸系统疾病的危险因素","authors":"Sophie Holcik, Lamia Hawayi, Naomi Dussah, Nick Barrowman, Nadya Ben Fadel, Bernard Thébaud, Sherri Lynne Katz","doi":"10.1002/ppul.71258","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bronchopulmonary dysplasia (BPD), defined as need for oxygen/respiratory support at 36 weeks gestational age (GA) is associated with increased risk of post-prematurity respiratory disease (PRD). We hypothesize that BPD, higher pCO2, and pulmonary hypertension (PH) before NICU discharge will predict PRD.</p><p><strong>Objectives: </strong>(1) Identify clinical factors before NICU discharge associated with PRD by 2 years of age; (2) Identify clinical factors associated with emergency room (ER) visits by 2 years of age; (3) Compare predictive performance for PRD of individual and multivariable clinical factors.</p><p><strong>Methodology: </strong>Children born < 29 weeks GA with ≥ 1 echocardiogram before NICU discharge at two tertiary centers were included. Retrospective chart review included clinical factors at NICU discharge, ER visits, and respiratory-related hospitalizations by 2 years. Analysis of predictors included logistic regression and ROC.</p><p><strong>Results: </strong>We included 125 premature infants, of whom 53 (42%) had BPD, and 24 (19%) experienced PRD. All who experienced PRD had BPD. More severe BPD (OR: 96.1, CI: 12.4, 12, 383), but not hypercapnia or PH, were associated with PRD. On ROC analysis, combination of BPD severity, pCO2 and PH demonstrated 70% chance of PRD (AUC: 0.68 (95% CI: 0.55, 0.81). Presence of ≥ 2 factors had sensitivity of 50% and specificity of 97% for prediction of PRD. Children with BPD had 2.6 times as many ER visits as those without.</p><p><strong>Conclusion: </strong>Combination of BPD severity, pCO2, and PH best predicted PRD. Identifying extremely preterm infants at high risk of developing PRD can guide counseling of families and early intervention.</p>","PeriodicalId":19932,"journal":{"name":"Pediatric Pulmonology","volume":"60 8","pages":"e71258"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372427/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors for Severe Respiratory Morbidity at 2 Years of Life in Children Born Extremely Preterm With Bronchopulmonary Dysplasia.\",\"authors\":\"Sophie Holcik, Lamia Hawayi, Naomi Dussah, Nick Barrowman, Nadya Ben Fadel, Bernard Thébaud, Sherri Lynne Katz\",\"doi\":\"10.1002/ppul.71258\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Bronchopulmonary dysplasia (BPD), defined as need for oxygen/respiratory support at 36 weeks gestational age (GA) is associated with increased risk of post-prematurity respiratory disease (PRD). We hypothesize that BPD, higher pCO2, and pulmonary hypertension (PH) before NICU discharge will predict PRD.</p><p><strong>Objectives: </strong>(1) Identify clinical factors before NICU discharge associated with PRD by 2 years of age; (2) Identify clinical factors associated with emergency room (ER) visits by 2 years of age; (3) Compare predictive performance for PRD of individual and multivariable clinical factors.</p><p><strong>Methodology: </strong>Children born < 29 weeks GA with ≥ 1 echocardiogram before NICU discharge at two tertiary centers were included. Retrospective chart review included clinical factors at NICU discharge, ER visits, and respiratory-related hospitalizations by 2 years. Analysis of predictors included logistic regression and ROC.</p><p><strong>Results: </strong>We included 125 premature infants, of whom 53 (42%) had BPD, and 24 (19%) experienced PRD. All who experienced PRD had BPD. More severe BPD (OR: 96.1, CI: 12.4, 12, 383), but not hypercapnia or PH, were associated with PRD. On ROC analysis, combination of BPD severity, pCO2 and PH demonstrated 70% chance of PRD (AUC: 0.68 (95% CI: 0.55, 0.81). Presence of ≥ 2 factors had sensitivity of 50% and specificity of 97% for prediction of PRD. Children with BPD had 2.6 times as many ER visits as those without.</p><p><strong>Conclusion: </strong>Combination of BPD severity, pCO2, and PH best predicted PRD. Identifying extremely preterm infants at high risk of developing PRD can guide counseling of families and early intervention.</p>\",\"PeriodicalId\":19932,\"journal\":{\"name\":\"Pediatric Pulmonology\",\"volume\":\"60 8\",\"pages\":\"e71258\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372427/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Pulmonology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ppul.71258\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Pulmonology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ppul.71258","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
Risk Factors for Severe Respiratory Morbidity at 2 Years of Life in Children Born Extremely Preterm With Bronchopulmonary Dysplasia.
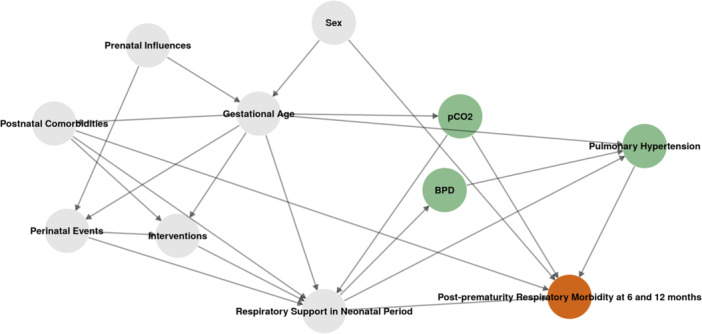
Background: Bronchopulmonary dysplasia (BPD), defined as need for oxygen/respiratory support at 36 weeks gestational age (GA) is associated with increased risk of post-prematurity respiratory disease (PRD). We hypothesize that BPD, higher pCO2, and pulmonary hypertension (PH) before NICU discharge will predict PRD.
Objectives: (1) Identify clinical factors before NICU discharge associated with PRD by 2 years of age; (2) Identify clinical factors associated with emergency room (ER) visits by 2 years of age; (3) Compare predictive performance for PRD of individual and multivariable clinical factors.
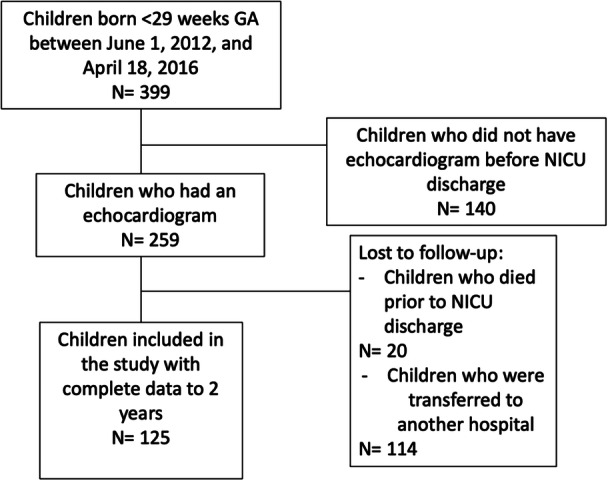
Methodology: Children born < 29 weeks GA with ≥ 1 echocardiogram before NICU discharge at two tertiary centers were included. Retrospective chart review included clinical factors at NICU discharge, ER visits, and respiratory-related hospitalizations by 2 years. Analysis of predictors included logistic regression and ROC.
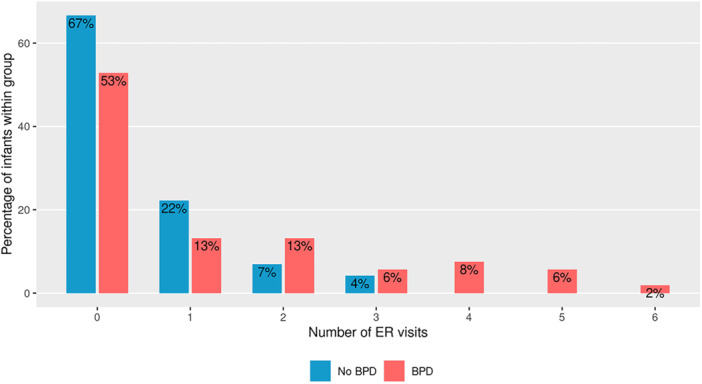
Results: We included 125 premature infants, of whom 53 (42%) had BPD, and 24 (19%) experienced PRD. All who experienced PRD had BPD. More severe BPD (OR: 96.1, CI: 12.4, 12, 383), but not hypercapnia or PH, were associated with PRD. On ROC analysis, combination of BPD severity, pCO2 and PH demonstrated 70% chance of PRD (AUC: 0.68 (95% CI: 0.55, 0.81). Presence of ≥ 2 factors had sensitivity of 50% and specificity of 97% for prediction of PRD. Children with BPD had 2.6 times as many ER visits as those without.
Conclusion: Combination of BPD severity, pCO2, and PH best predicted PRD. Identifying extremely preterm infants at high risk of developing PRD can guide counseling of families and early intervention.
期刊介绍:
Pediatric Pulmonology (PPUL) is the foremost global journal studying the respiratory system in disease and in health as it develops from intrauterine life though adolescence to adulthood. Combining explicit and informative analysis of clinical as well as basic scientific research, PPUL provides a look at the many facets of respiratory system disorders in infants and children, ranging from pathological anatomy, developmental issues, and pathophysiology to infectious disease, asthma, cystic fibrosis, and airborne toxins. Focused attention is given to the reporting of diagnostic and therapeutic methods for neonates, preschool children, and adolescents, the enduring effects of childhood respiratory diseases, and newly described infectious diseases.
PPUL concentrates on subject matters of crucial interest to specialists preparing for the Pediatric Subspecialty Examinations in the United States and other countries. With its attentive coverage and extensive clinical data, this journal is a principle source for pediatricians in practice and in training and a must have for all pediatric pulmonologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


