Zofia Kachlik, Wiesław Jerzy Cubała, Michał Walaszek, Michał Pastuszak, Krzysztof Pastuszak, Aleksander Kwaśny
{"title":"难治性双相抑郁症对氯胺酮无反应。","authors":"Zofia Kachlik, Wiesław Jerzy Cubała, Michał Walaszek, Michał Pastuszak, Krzysztof Pastuszak, Aleksander Kwaśny","doi":"10.1002/npr2.70038","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Ketamine is a prototypical rapid-acting antidepressant for treatment-resistant bipolar depression (TRBD), yet many patients do not achieve a meaningful response. This study explored features of ketamine nonresponse in TRBD.</p><p><strong>Methods: </strong>In a post hoc analysis of a naturalistic study, 35 TRBD patients received a four-week ketamine regimen (intravenous 0.5 mg/kg or oral 2.0/2.5 mg/kg). Response was measured using the Montgomery-Åsberg Depression Rating Scale, and baseline sociodemographic and clinical features were compared between responders and nonresponders.</p><p><strong>Results: </strong>Fourteen patients (40%) were nonresponders. They had a higher median number of psychiatric comorbidities (2 vs. 1; p = 0.0366), were more likely to have any psychiatric comorbidity (78.6% vs. 33.3%; p = 0.0153), and had greater prior benzodiazepine use (64.3% vs. 23.8%; p = 0.0332). No significant links emerged between individual comorbidities or baseline suicidality and response.</p><p><strong>Conclusion: </strong>Ketamine demonstrates a favorable safety and tolerability profile for short time use in TRBD regardless of isolated baseline characteristics, although a more severe comorbidity burden and benzodiazepine use appear to be associated with nonresponse.</p><p><strong>Trial registration: </strong>NCT04226963 and NCT05565352.</p>","PeriodicalId":19137,"journal":{"name":"Neuropsychopharmacology Reports","volume":"45 3","pages":"e70038"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277043/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nonresponse to Ketamine in Treatment-Resistant Bipolar Depression.\",\"authors\":\"Zofia Kachlik, Wiesław Jerzy Cubała, Michał Walaszek, Michał Pastuszak, Krzysztof Pastuszak, Aleksander Kwaśny\",\"doi\":\"10.1002/npr2.70038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Ketamine is a prototypical rapid-acting antidepressant for treatment-resistant bipolar depression (TRBD), yet many patients do not achieve a meaningful response. This study explored features of ketamine nonresponse in TRBD.</p><p><strong>Methods: </strong>In a post hoc analysis of a naturalistic study, 35 TRBD patients received a four-week ketamine regimen (intravenous 0.5 mg/kg or oral 2.0/2.5 mg/kg). Response was measured using the Montgomery-Åsberg Depression Rating Scale, and baseline sociodemographic and clinical features were compared between responders and nonresponders.</p><p><strong>Results: </strong>Fourteen patients (40%) were nonresponders. They had a higher median number of psychiatric comorbidities (2 vs. 1; p = 0.0366), were more likely to have any psychiatric comorbidity (78.6% vs. 33.3%; p = 0.0153), and had greater prior benzodiazepine use (64.3% vs. 23.8%; p = 0.0332). No significant links emerged between individual comorbidities or baseline suicidality and response.</p><p><strong>Conclusion: </strong>Ketamine demonstrates a favorable safety and tolerability profile for short time use in TRBD regardless of isolated baseline characteristics, although a more severe comorbidity burden and benzodiazepine use appear to be associated with nonresponse.</p><p><strong>Trial registration: </strong>NCT04226963 and NCT05565352.</p>\",\"PeriodicalId\":19137,\"journal\":{\"name\":\"Neuropsychopharmacology Reports\",\"volume\":\"45 3\",\"pages\":\"e70038\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277043/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neuropsychopharmacology Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/npr2.70038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuropsychopharmacology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/npr2.70038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
Nonresponse to Ketamine in Treatment-Resistant Bipolar Depression.
Objectives: Ketamine is a prototypical rapid-acting antidepressant for treatment-resistant bipolar depression (TRBD), yet many patients do not achieve a meaningful response. This study explored features of ketamine nonresponse in TRBD.
Methods: In a post hoc analysis of a naturalistic study, 35 TRBD patients received a four-week ketamine regimen (intravenous 0.5 mg/kg or oral 2.0/2.5 mg/kg). Response was measured using the Montgomery-Åsberg Depression Rating Scale, and baseline sociodemographic and clinical features were compared between responders and nonresponders.
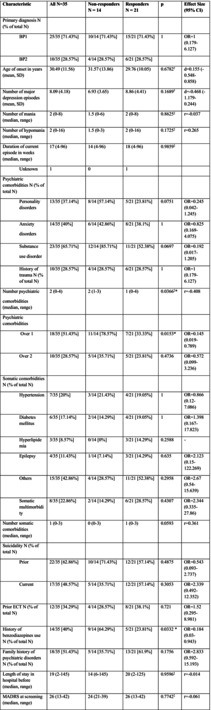
Results: Fourteen patients (40%) were nonresponders. They had a higher median number of psychiatric comorbidities (2 vs. 1; p = 0.0366), were more likely to have any psychiatric comorbidity (78.6% vs. 33.3%; p = 0.0153), and had greater prior benzodiazepine use (64.3% vs. 23.8%; p = 0.0332). No significant links emerged between individual comorbidities or baseline suicidality and response.
Conclusion: Ketamine demonstrates a favorable safety and tolerability profile for short time use in TRBD regardless of isolated baseline characteristics, although a more severe comorbidity burden and benzodiazepine use appear to be associated with nonresponse.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


