Jasper Koolwijk, Mileen van de Kar, Brittney A van der Woude, Marcel van 't Veer, Harm Jan de Grooth, Harry J G M Crijns, Lukas R C Dekker, R Arthur Bouwman, Olaf L Cremer, Ashley J R de Bie, Luuk C Otterspoor
{"title":"危重患者诱发性心房颤动的抗凝和血栓栓塞风险:系统回顾和荟萃分析","authors":"Jasper Koolwijk, Mileen van de Kar, Brittney A van der Woude, Marcel van 't Veer, Harm Jan de Grooth, Harry J G M Crijns, Lukas R C Dekker, R Arthur Bouwman, Olaf L Cremer, Ashley J R de Bie, Luuk C Otterspoor","doi":"10.1007/s12471-025-01978-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In critically ill patients with trigger-induced atrial fibrillation, there are no definitive recommendations on the use of anticoagulation. This study aimed to evaluate the association between anticoagulation therapy and outcomes (i.e. thromboembolism, bleeding and mortality) and examine prescription patterns in high-risk individuals based on CHA<sub>2</sub>DS<sub>2</sub>-VASc scores.</p><p><strong>Methods: </strong>A systematic search was conducted to identify studies reporting on anticoagulation prescription, thromboembolism, bleeding, and mortality. Anticoagulation rates and CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were correlated, and a meta-analysis was conducted to compare short- and long-term outcomes.</p><p><strong>Results: </strong>Anticoagulation prescription rates ranged from 3 to 86%; in over 50% of patients, CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were ≥ 2 (n = 28 studies). A meta-analysis of eight observational studies, in which 95% of patients had sepsis/infection as the precipitant, demonstrated no association between anticoagulation and reduced short-term thromboembolism (OR 0.89, 95% CI 0.61-1.28) or increased bleeding (OR 1.05, 95% CI 0.90-1.22). Short-term mortality was lower in the anticoagulation group (OR 0.54, 95% CI 0.39-0.75), but a higher long-term thromboembolic risk was observed (OR 1.45, 95% CI 1.04-2.03).</p><p><strong>Conclusion: </strong>The prescription of anticoagulation in critically ill patients with TIAF is highly variable. There is no clear evidence of benefit or harm, and neither routine use nor systematic omission is supported.</p>","PeriodicalId":18952,"journal":{"name":"Netherlands Heart Journal","volume":" ","pages":"290-298"},"PeriodicalIF":2.0000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454756/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anticoagulation and thromboembolic risk in critically ill patients with trigger-induced atrial fibrillation-A systematic review and meta-analysis.\",\"authors\":\"Jasper Koolwijk, Mileen van de Kar, Brittney A van der Woude, Marcel van 't Veer, Harm Jan de Grooth, Harry J G M Crijns, Lukas R C Dekker, R Arthur Bouwman, Olaf L Cremer, Ashley J R de Bie, Luuk C Otterspoor\",\"doi\":\"10.1007/s12471-025-01978-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>In critically ill patients with trigger-induced atrial fibrillation, there are no definitive recommendations on the use of anticoagulation. This study aimed to evaluate the association between anticoagulation therapy and outcomes (i.e. thromboembolism, bleeding and mortality) and examine prescription patterns in high-risk individuals based on CHA<sub>2</sub>DS<sub>2</sub>-VASc scores.</p><p><strong>Methods: </strong>A systematic search was conducted to identify studies reporting on anticoagulation prescription, thromboembolism, bleeding, and mortality. Anticoagulation rates and CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were correlated, and a meta-analysis was conducted to compare short- and long-term outcomes.</p><p><strong>Results: </strong>Anticoagulation prescription rates ranged from 3 to 86%; in over 50% of patients, CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were ≥ 2 (n = 28 studies). A meta-analysis of eight observational studies, in which 95% of patients had sepsis/infection as the precipitant, demonstrated no association between anticoagulation and reduced short-term thromboembolism (OR 0.89, 95% CI 0.61-1.28) or increased bleeding (OR 1.05, 95% CI 0.90-1.22). Short-term mortality was lower in the anticoagulation group (OR 0.54, 95% CI 0.39-0.75), but a higher long-term thromboembolic risk was observed (OR 1.45, 95% CI 1.04-2.03).</p><p><strong>Conclusion: </strong>The prescription of anticoagulation in critically ill patients with TIAF is highly variable. There is no clear evidence of benefit or harm, and neither routine use nor systematic omission is supported.</p>\",\"PeriodicalId\":18952,\"journal\":{\"name\":\"Netherlands Heart Journal\",\"volume\":\" \",\"pages\":\"290-298\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454756/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Netherlands Heart Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12471-025-01978-9\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Netherlands Heart Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12471-025-01978-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
在危重患者的触发性心房颤动,没有明确的建议使用抗凝。本研究旨在评估抗凝治疗与预后(即血栓栓塞、出血和死亡率)之间的关系,并根据CHA2DS2-VASc评分检查高危人群的处方模式。方法:系统检索了关于抗凝处方、血栓栓塞、出血和死亡率的研究报告。抗凝率与CHA2DS2-VASc评分相关,并进行meta分析比较短期和长期结果。结果:抗凝处方率为3% ~ 86%;超过50%的患者CHA2DS2-VASc评分≥ 2 (n = 28项研究)。一项对8项观察性研究的荟萃分析显示,抗凝与减少短期血栓栓塞(OR 0.89, 95% CI 0.61-1.28)或增加出血(OR 1.05, 95% CI 0.90-1.22)之间没有关联,其中95%的患者有败血症/感染作为沉淀因素。抗凝组短期死亡率较低(OR 0.54, 95% CI 0.39-0.75),但观察到较高的长期血栓栓塞风险(OR 1.45, 95% CI 1.04-2.03)。结论:重症TIAF患者抗凝处方变化较大。没有明确的证据表明其有益或有害,既不支持常规使用,也不支持系统性遗漏。
Anticoagulation and thromboembolic risk in critically ill patients with trigger-induced atrial fibrillation-A systematic review and meta-analysis.
Introduction: In critically ill patients with trigger-induced atrial fibrillation, there are no definitive recommendations on the use of anticoagulation. This study aimed to evaluate the association between anticoagulation therapy and outcomes (i.e. thromboembolism, bleeding and mortality) and examine prescription patterns in high-risk individuals based on CHA2DS2-VASc scores.
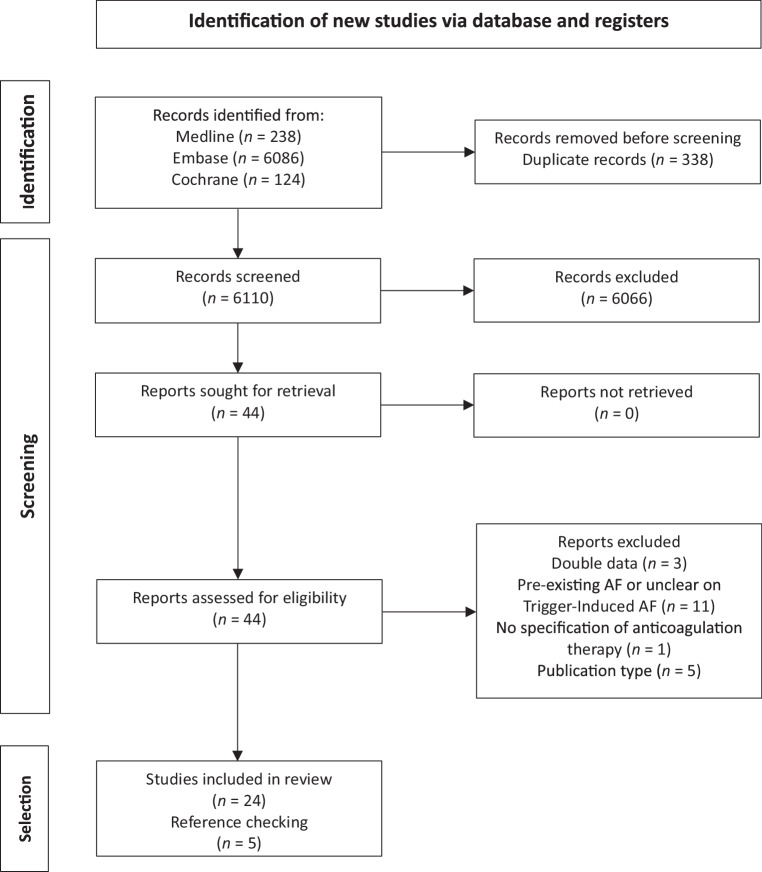
Methods: A systematic search was conducted to identify studies reporting on anticoagulation prescription, thromboembolism, bleeding, and mortality. Anticoagulation rates and CHA2DS2-VASc scores were correlated, and a meta-analysis was conducted to compare short- and long-term outcomes.
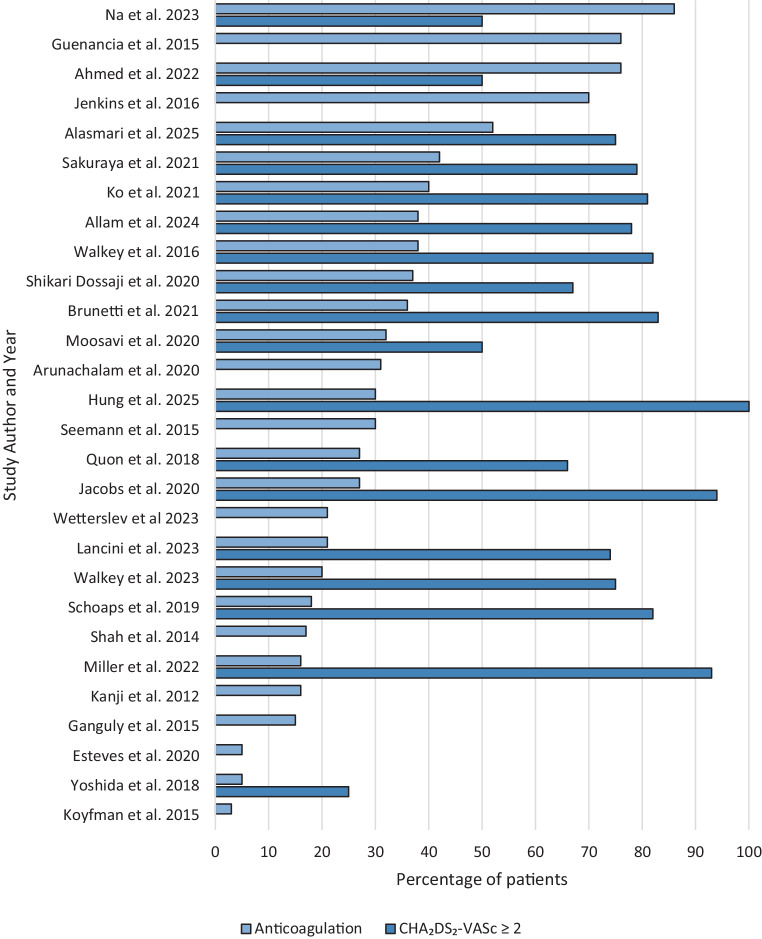
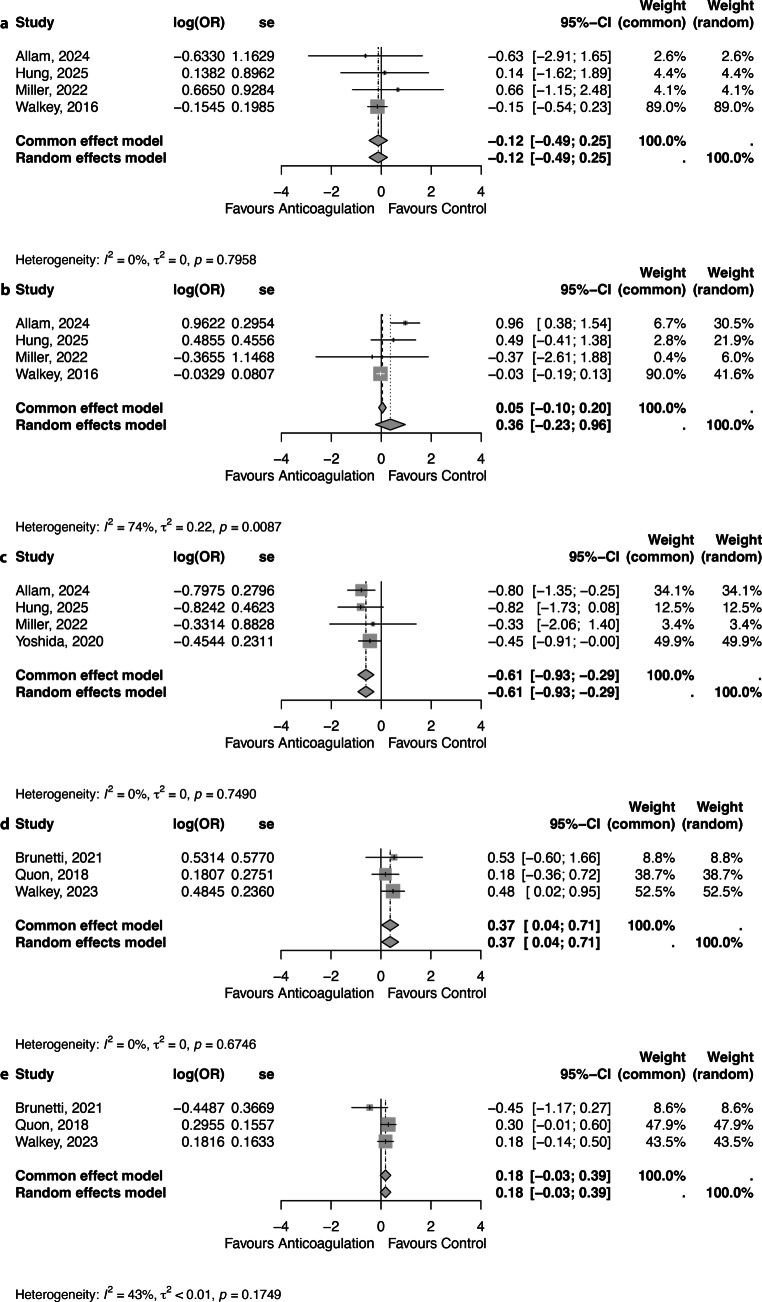
Results: Anticoagulation prescription rates ranged from 3 to 86%; in over 50% of patients, CHA2DS2-VASc scores were ≥ 2 (n = 28 studies). A meta-analysis of eight observational studies, in which 95% of patients had sepsis/infection as the precipitant, demonstrated no association between anticoagulation and reduced short-term thromboembolism (OR 0.89, 95% CI 0.61-1.28) or increased bleeding (OR 1.05, 95% CI 0.90-1.22). Short-term mortality was lower in the anticoagulation group (OR 0.54, 95% CI 0.39-0.75), but a higher long-term thromboembolic risk was observed (OR 1.45, 95% CI 1.04-2.03).
Conclusion: The prescription of anticoagulation in critically ill patients with TIAF is highly variable. There is no clear evidence of benefit or harm, and neither routine use nor systematic omission is supported.
期刊介绍:
The scope of the Netherlands Heart Journal is to contribute to the national and international literature by publishing scientific papers in the field of cardiovascular medicine. It also provides a platform for Continuing Medical Education for cardiologists and those in training for the speciality of cardiology in the Netherlands.
The Netherlands Heart Journal is made available to cardiologists, cardiologists in training, cardiopulmonary surgeons, cardiopulmonary surgeons in training, internists and paediatric cardiologists. The journal is the official journal of the Netherlands Society of Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


