Nilüfer Akgün, Yavuz Emre Şükür, Batuhan Aslan, Necati Berk Kaplan, Onur Alp Acun, Batuhan Özmen, Murat Sönmezer, Bülent Berker, Cem Somer Atabekoğlu, Ruşen Aytaç
{"title":"在辅助生殖技术周期中,波塞冬第3组和第4组反应不良者最终卵母细胞成熟的最佳前导卵泡大小。","authors":"Nilüfer Akgün, Yavuz Emre Şükür, Batuhan Aslan, Necati Berk Kaplan, Onur Alp Acun, Batuhan Özmen, Murat Sönmezer, Bülent Berker, Cem Somer Atabekoğlu, Ruşen Aytaç","doi":"10.4274/jtgga.galenos.2025.2025-7-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this retrospective cohort study was to evaluate the relationship between leading follicle size at the time of human chorionic gonadotropin (hCG) trigger and live birth rates in Patient-Oriented Strategies Encompassing Individualised Oocyte Number (POSEIDON) groups 3 and 4 undergoing assisted reproductive technology cycles using a gonadotropin releasing hormone (GnRH) antagonist protocol. The objective was to identify the optimal leading follicle size for maximizing live birth outcomes in this challenging patient population.</p><p><strong>Material and methods: </strong>This retrospective cohort study included POSEIDON groups 3 and 4 poor responders aged 20-42 years undergoing intracytoplasmic sperm injection with GnRH antagonist protocol between January 2015 and July 2021. Patients were categorized based on the occurrence of premature ovulation. The primary outcome measures were number of oocytes retrieved, number of metaphase II (MII) oocytes, MII oocyte ratio and follicle oocyte index (FOI). These outcomes were compared across different leading follicle size categories at the time of hCG trigger.</p><p><strong>Results: </strong>Among the 294 subjects included, 47 (16.2%) had premature ovulation between the trigger and oocyte pick-up days. The mean size of the leading follicle on the day of trigger was significantly higher in the premature ovulation group (19.8±2.4 mm vs.18.7±2 mm, respectively; p<0.001). Multivariate logistic regression analyses identified baseline luteinizing hormone [odds ratio (OR) 1.144, 95% confidence interval (CI) 1.052-1.243; p=0.002], number of follicles >11 mm on the day of trigger (OR 0.580, 95% CI 0.438-0.767; p<0.001), and leading follicle size (OR 1.361, 95% CI 1.130-1.641; p=0.001) as independent predictors of premature ovulation. The FOI and MII/antral follicle count ratios peaked when the leading follicle size was between 16-17 mm.</p><p><strong>Conclusion: </strong>Individualized triggering based on leading follicle size may provide optimal oocyte retrieval after ovarian stimulation in POSEIDON expected poor responders. While a late trigger may result in premature ovulation, an early trigger may also result in less MII. Triggering when the leading follicle size is between 16.5 and 17 mm may help to prevent these negative outcomes and achieve optimal cycle outcome.</p>","PeriodicalId":17440,"journal":{"name":"Journal of the Turkish German Gynecological Association","volume":"26 3","pages":"195-203"},"PeriodicalIF":1.4000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406972/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimal leading follicle size for final oocyte maturation in POSEIDON group 3 and 4 poor responders undergoing assisted reproductive technology cycles.\",\"authors\":\"Nilüfer Akgün, Yavuz Emre Şükür, Batuhan Aslan, Necati Berk Kaplan, Onur Alp Acun, Batuhan Özmen, Murat Sönmezer, Bülent Berker, Cem Somer Atabekoğlu, Ruşen Aytaç\",\"doi\":\"10.4274/jtgga.galenos.2025.2025-7-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim of this retrospective cohort study was to evaluate the relationship between leading follicle size at the time of human chorionic gonadotropin (hCG) trigger and live birth rates in Patient-Oriented Strategies Encompassing Individualised Oocyte Number (POSEIDON) groups 3 and 4 undergoing assisted reproductive technology cycles using a gonadotropin releasing hormone (GnRH) antagonist protocol. The objective was to identify the optimal leading follicle size for maximizing live birth outcomes in this challenging patient population.</p><p><strong>Material and methods: </strong>This retrospective cohort study included POSEIDON groups 3 and 4 poor responders aged 20-42 years undergoing intracytoplasmic sperm injection with GnRH antagonist protocol between January 2015 and July 2021. Patients were categorized based on the occurrence of premature ovulation. The primary outcome measures were number of oocytes retrieved, number of metaphase II (MII) oocytes, MII oocyte ratio and follicle oocyte index (FOI). These outcomes were compared across different leading follicle size categories at the time of hCG trigger.</p><p><strong>Results: </strong>Among the 294 subjects included, 47 (16.2%) had premature ovulation between the trigger and oocyte pick-up days. The mean size of the leading follicle on the day of trigger was significantly higher in the premature ovulation group (19.8±2.4 mm vs.18.7±2 mm, respectively; p<0.001). Multivariate logistic regression analyses identified baseline luteinizing hormone [odds ratio (OR) 1.144, 95% confidence interval (CI) 1.052-1.243; p=0.002], number of follicles >11 mm on the day of trigger (OR 0.580, 95% CI 0.438-0.767; p<0.001), and leading follicle size (OR 1.361, 95% CI 1.130-1.641; p=0.001) as independent predictors of premature ovulation. The FOI and MII/antral follicle count ratios peaked when the leading follicle size was between 16-17 mm.</p><p><strong>Conclusion: </strong>Individualized triggering based on leading follicle size may provide optimal oocyte retrieval after ovarian stimulation in POSEIDON expected poor responders. While a late trigger may result in premature ovulation, an early trigger may also result in less MII. Triggering when the leading follicle size is between 16.5 and 17 mm may help to prevent these negative outcomes and achieve optimal cycle outcome.</p>\",\"PeriodicalId\":17440,\"journal\":{\"name\":\"Journal of the Turkish German Gynecological Association\",\"volume\":\"26 3\",\"pages\":\"195-203\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406972/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Turkish German Gynecological Association\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4274/jtgga.galenos.2025.2025-7-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Turkish German Gynecological Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/jtgga.galenos.2025.2025-7-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:本回顾性队列研究的目的是评估在以患者为导向的包括个体化卵母细胞数量(POSEIDON)的策略中,在使用促性腺激素释放激素(GnRH)拮抗剂方案进行辅助生殖技术周期的第3组和第4组中,人绒毛膜促性腺激素(hCG)触发时先导卵泡大小与活产率之间的关系。目的是确定在这个具有挑战性的患者群体中最大限度地提高活产结果的最佳先导卵泡大小。材料和方法:该回顾性队列研究纳入了POSEIDON 3组和4组,年龄20-42岁,在2015年1月至2021年7月期间接受GnRH拮抗剂方案的胞浆内单精子注射。根据早泄的发生情况对患者进行分类。主要观察指标为回收卵母细胞数、中期II期(MII)卵母细胞数、中期II期卵母细胞比率和卵泡卵母细胞指数(FOI)。在hCG触发时,这些结果在不同主要卵泡大小类别中进行了比较。结果:294例受试者中,47例(16.2%)在触发日和取卵日之间发生早排卵。早排卵组触发当天先导卵泡的平均大小显著高于对照组(分别为19.8±2.4 mm和18.7±2 mm);触发当天先导卵泡的平均大小为11 mm (OR 0.580, 95% CI 0.438-0.767)。结论:基于先导卵泡大小的个体化触发可能为波塞冬预期不良应答者提供卵巢刺激后最佳的卵母细胞回收。虽然晚触发可能导致早泄,但早触发也可能导致MII减少。当主要卵泡大小在16.5和17毫米之间时触发可能有助于防止这些负面结果并实现最佳周期结果。
Optimal leading follicle size for final oocyte maturation in POSEIDON group 3 and 4 poor responders undergoing assisted reproductive technology cycles.
Objective: The aim of this retrospective cohort study was to evaluate the relationship between leading follicle size at the time of human chorionic gonadotropin (hCG) trigger and live birth rates in Patient-Oriented Strategies Encompassing Individualised Oocyte Number (POSEIDON) groups 3 and 4 undergoing assisted reproductive technology cycles using a gonadotropin releasing hormone (GnRH) antagonist protocol. The objective was to identify the optimal leading follicle size for maximizing live birth outcomes in this challenging patient population.
Material and methods: This retrospective cohort study included POSEIDON groups 3 and 4 poor responders aged 20-42 years undergoing intracytoplasmic sperm injection with GnRH antagonist protocol between January 2015 and July 2021. Patients were categorized based on the occurrence of premature ovulation. The primary outcome measures were number of oocytes retrieved, number of metaphase II (MII) oocytes, MII oocyte ratio and follicle oocyte index (FOI). These outcomes were compared across different leading follicle size categories at the time of hCG trigger.
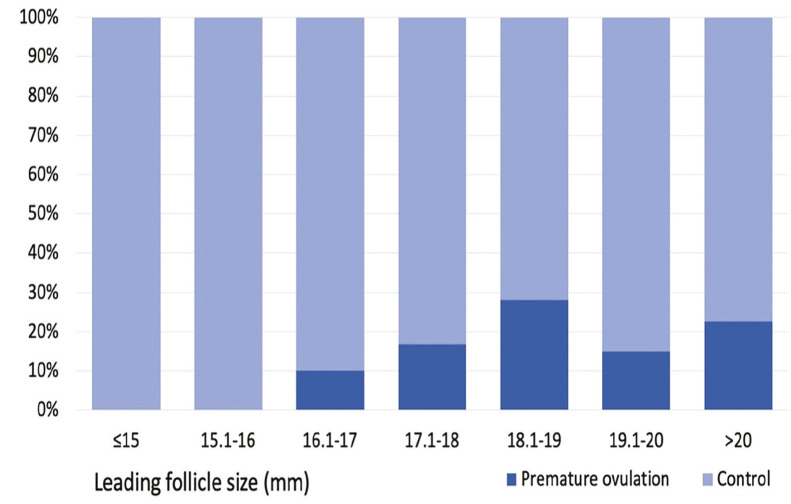
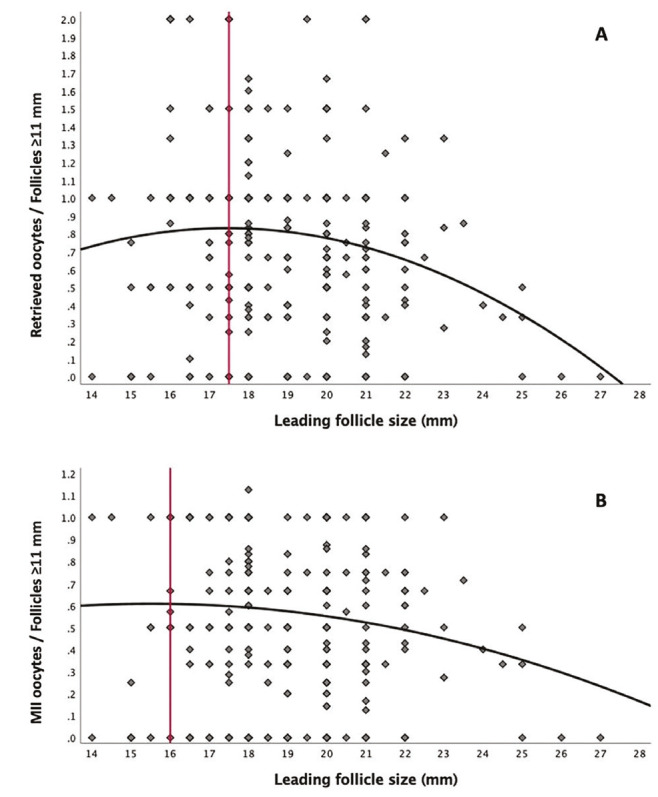
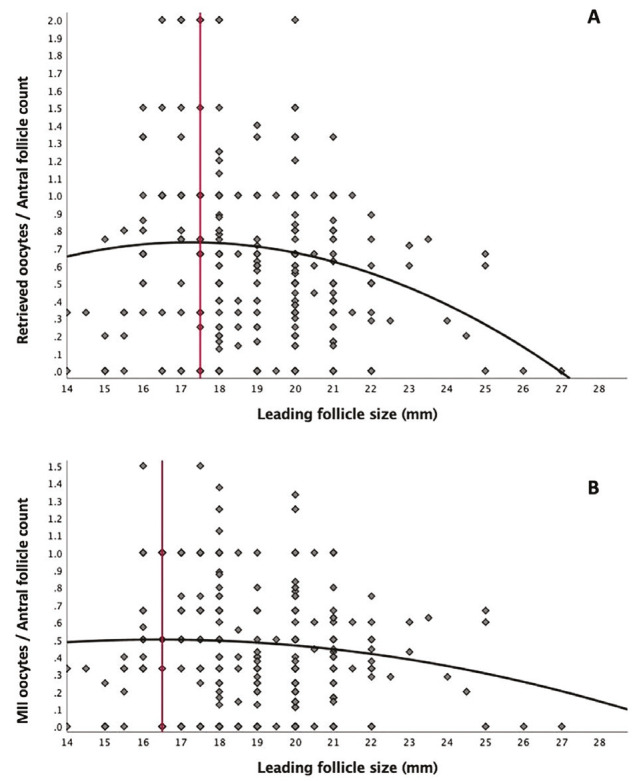
Results: Among the 294 subjects included, 47 (16.2%) had premature ovulation between the trigger and oocyte pick-up days. The mean size of the leading follicle on the day of trigger was significantly higher in the premature ovulation group (19.8±2.4 mm vs.18.7±2 mm, respectively; p<0.001). Multivariate logistic regression analyses identified baseline luteinizing hormone [odds ratio (OR) 1.144, 95% confidence interval (CI) 1.052-1.243; p=0.002], number of follicles >11 mm on the day of trigger (OR 0.580, 95% CI 0.438-0.767; p<0.001), and leading follicle size (OR 1.361, 95% CI 1.130-1.641; p=0.001) as independent predictors of premature ovulation. The FOI and MII/antral follicle count ratios peaked when the leading follicle size was between 16-17 mm.
Conclusion: Individualized triggering based on leading follicle size may provide optimal oocyte retrieval after ovarian stimulation in POSEIDON expected poor responders. While a late trigger may result in premature ovulation, an early trigger may also result in less MII. Triggering when the leading follicle size is between 16.5 and 17 mm may help to prevent these negative outcomes and achieve optimal cycle outcome.
期刊介绍:
Journal of the Turkish-German Gynecological Association is the official, open access publication of the Turkish-German Gynecological Education and Research Foundation and Turkish-German Gynecological Association and is published quarterly on March, June, September and December. It is an independent peer-reviewed international journal printed in English language. Manuscripts are reviewed in accordance with “double-blind peer review” process for both reviewers and authors. The target audience of Journal of the Turkish-German Gynecological Association includes gynecologists and primary care physicians interested in gynecology practice. It publishes original works on all aspects of obstertrics and gynecology. The aim of Journal of the Turkish-German Gynecological Association is to publish high quality original research articles. In addition to research articles, reviews, editorials, letters to the editor, diagnostic puzzle are also published. Suggestions for new books are also welcomed. Journal of the Turkish-German Gynecological Association does not charge any fee for article submission or processing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


