{"title":"1例BRAF v600e突变的转移性结直肠癌患者接受恩可非尼、比尼美替尼和西妥昔单抗治疗的严重症状性心功能障碍","authors":"Masahiro Kondo, Yukiko Nagao, Shohei Hayashi, Eri Wakita, Masato Noda, Itsuki Okada, Chiharu Wachino, Keiko Yamada-Nishide, Masayuki Hori, Yuji Hotta, Yoichi Matsuo, Yoko Furukawa-Hibi","doi":"10.1186/s40780-025-00480-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>V-Raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations are present in approximately 5% of Japanese patients with colorectal cancer (CRC) who receive BRAF-targeted triplet therapy, consisting of encorafenib (a BRAF inhibitor), binimetinib (a mitogen-activated protein kinase inhibitor [MEKi]), and cetuximab. This combination therapy is associated with an increased risk of cardiac dysfunction (CD), primarily attributed to MEKi. However, the detailed clinical course of this adverse event remains unclear. Here, we report a case of severe symptomatic CD that developed during this triplet therapy.</p><p><strong>Case presentation: </strong>The patient was a 70-year-old Japanese man diagnosed with BRAF-mutated CRC with multiple metastases. BRAF-targeted triplet therapy was initiated as a third-line treatment. His baseline left ventricular ejection fraction (LVEF) was 66% and he had no history of heart disease. On Day 106, a pharmacist conducting the patient's consultation suspected CD associated with binimetinib because of symptoms such as deterioration of general condition and dyspnea. The pharmacist immediately recommended an echocardiography that revealed a significant decline in LVEF to 33%. The patient was referred to a cardiologist and treatment with enalapril, followed by bisoprolol, was initiated while triplet therapy was discontinued. Within 1 week of treatment interruption, the patient's general condition improved rapidly and his symptoms resolved. Therefore, cancer treatment was resumed as doublet therapy without binimetinib. Under close multidisciplinary monitoring, no recurrence of CD symptoms was observed. Doublet therapy was continued until Day 168, when disease progression occurred. This exceeded the median progression-free survival reported in the phase III BEACON-CRC trial.</p><p><strong>Conclusions: </strong>This case highlights two crucial insights into BRAF/MEK inhibitor-associated CD. First, even severe symptomatic CD can be effectively managed and reversed upon immediate discontinuation of binimetinib and initiation of cardiotropic medications. Second, in such a severe case, rapid recovery is observed. Once stabilized, BRAF-targeted treatment could be continued as doublet therapy without binimetinib to ensure safety and disease control. However, regular echocardiographic surveillance is essential, with an interval shorter than 4 months, based on the clinical course of this case. Additionally, early recognition of CD may be improved by closely monitoring patients' symptoms and complaints through a multidisciplinary approach.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"11 1","pages":"80"},"PeriodicalIF":1.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400612/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe symptomatic cardiac dysfunction in a patient with BRAF V600E-mutated metastatic colorectal cancer treated with encorafenib, binimetinib, and cetuximab: a case report.\",\"authors\":\"Masahiro Kondo, Yukiko Nagao, Shohei Hayashi, Eri Wakita, Masato Noda, Itsuki Okada, Chiharu Wachino, Keiko Yamada-Nishide, Masayuki Hori, Yuji Hotta, Yoichi Matsuo, Yoko Furukawa-Hibi\",\"doi\":\"10.1186/s40780-025-00480-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>V-Raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations are present in approximately 5% of Japanese patients with colorectal cancer (CRC) who receive BRAF-targeted triplet therapy, consisting of encorafenib (a BRAF inhibitor), binimetinib (a mitogen-activated protein kinase inhibitor [MEKi]), and cetuximab. This combination therapy is associated with an increased risk of cardiac dysfunction (CD), primarily attributed to MEKi. However, the detailed clinical course of this adverse event remains unclear. Here, we report a case of severe symptomatic CD that developed during this triplet therapy.</p><p><strong>Case presentation: </strong>The patient was a 70-year-old Japanese man diagnosed with BRAF-mutated CRC with multiple metastases. BRAF-targeted triplet therapy was initiated as a third-line treatment. His baseline left ventricular ejection fraction (LVEF) was 66% and he had no history of heart disease. On Day 106, a pharmacist conducting the patient's consultation suspected CD associated with binimetinib because of symptoms such as deterioration of general condition and dyspnea. The pharmacist immediately recommended an echocardiography that revealed a significant decline in LVEF to 33%. The patient was referred to a cardiologist and treatment with enalapril, followed by bisoprolol, was initiated while triplet therapy was discontinued. Within 1 week of treatment interruption, the patient's general condition improved rapidly and his symptoms resolved. Therefore, cancer treatment was resumed as doublet therapy without binimetinib. Under close multidisciplinary monitoring, no recurrence of CD symptoms was observed. Doublet therapy was continued until Day 168, when disease progression occurred. This exceeded the median progression-free survival reported in the phase III BEACON-CRC trial.</p><p><strong>Conclusions: </strong>This case highlights two crucial insights into BRAF/MEK inhibitor-associated CD. First, even severe symptomatic CD can be effectively managed and reversed upon immediate discontinuation of binimetinib and initiation of cardiotropic medications. Second, in such a severe case, rapid recovery is observed. Once stabilized, BRAF-targeted treatment could be continued as doublet therapy without binimetinib to ensure safety and disease control. However, regular echocardiographic surveillance is essential, with an interval shorter than 4 months, based on the clinical course of this case. Additionally, early recognition of CD may be improved by closely monitoring patients' symptoms and complaints through a multidisciplinary approach.</p>\",\"PeriodicalId\":16730,\"journal\":{\"name\":\"Journal of Pharmaceutical Health Care and Sciences\",\"volume\":\"11 1\",\"pages\":\"80\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400612/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Health Care and Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40780-025-00480-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-025-00480-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Severe symptomatic cardiac dysfunction in a patient with BRAF V600E-mutated metastatic colorectal cancer treated with encorafenib, binimetinib, and cetuximab: a case report.
Background: V-Raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations are present in approximately 5% of Japanese patients with colorectal cancer (CRC) who receive BRAF-targeted triplet therapy, consisting of encorafenib (a BRAF inhibitor), binimetinib (a mitogen-activated protein kinase inhibitor [MEKi]), and cetuximab. This combination therapy is associated with an increased risk of cardiac dysfunction (CD), primarily attributed to MEKi. However, the detailed clinical course of this adverse event remains unclear. Here, we report a case of severe symptomatic CD that developed during this triplet therapy.
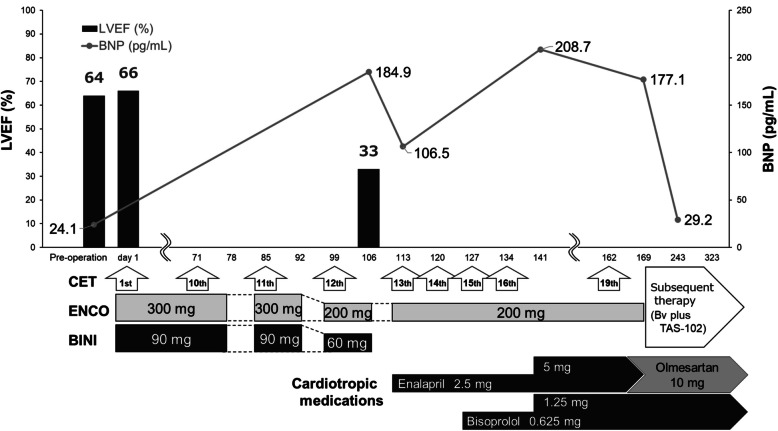
Case presentation: The patient was a 70-year-old Japanese man diagnosed with BRAF-mutated CRC with multiple metastases. BRAF-targeted triplet therapy was initiated as a third-line treatment. His baseline left ventricular ejection fraction (LVEF) was 66% and he had no history of heart disease. On Day 106, a pharmacist conducting the patient's consultation suspected CD associated with binimetinib because of symptoms such as deterioration of general condition and dyspnea. The pharmacist immediately recommended an echocardiography that revealed a significant decline in LVEF to 33%. The patient was referred to a cardiologist and treatment with enalapril, followed by bisoprolol, was initiated while triplet therapy was discontinued. Within 1 week of treatment interruption, the patient's general condition improved rapidly and his symptoms resolved. Therefore, cancer treatment was resumed as doublet therapy without binimetinib. Under close multidisciplinary monitoring, no recurrence of CD symptoms was observed. Doublet therapy was continued until Day 168, when disease progression occurred. This exceeded the median progression-free survival reported in the phase III BEACON-CRC trial.
Conclusions: This case highlights two crucial insights into BRAF/MEK inhibitor-associated CD. First, even severe symptomatic CD can be effectively managed and reversed upon immediate discontinuation of binimetinib and initiation of cardiotropic medications. Second, in such a severe case, rapid recovery is observed. Once stabilized, BRAF-targeted treatment could be continued as doublet therapy without binimetinib to ensure safety and disease control. However, regular echocardiographic surveillance is essential, with an interval shorter than 4 months, based on the clinical course of this case. Additionally, early recognition of CD may be improved by closely monitoring patients' symptoms and complaints through a multidisciplinary approach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


