Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte
{"title":"2019冠状病毒病大流行期间采用的替代护理途径对泰国一家三级护理医院非传染性疾病管理的影响。","authors":"Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte","doi":"10.1080/20523211.2025.2544644","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of non-communicable diseases (NCDs), including hypertension (HT) and diabetes mellitus (DM), was significantly impacted by the COVID-19 pandemic. Many institutions adopted alternative care pathways, e.g. pharmacy at home (PAH), and the deferred care (DC). While PAH has been studied for clinical outcomes, evaluation of the DC remains limited. Consequently, this study evaluates both the clinical and economic outcomes of the PAH and DC as alternatives to usual care.</p><p><strong>Method: </strong>A retrospective study was conducted at a tertiary care hospital in Thailand from 1 July 2021, to 30 June 2023. Data from outpatients with HT and DM were classified into PAH, DC, or discharged home with follow-up at the hospital. Clinical outcomes included changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), and fasting blood sugar (FBS), calculated from baseline to follow-up. Economic outcome was the cost of illness (COI) per patient visit. Multivariate multilevel mixed-effects linear regression assessed clinical outcomes, while log-linear regression evaluated economic outcome.</p><p><strong>Results: </strong>There were 3,518 patients in the pandemic period and 4,135 patients in the post pandemic period. There was no statistically significant impact of PAH and DC on changes in SBP, DBP, and FBS. However, both care pathways significantly reduced COI during both periods (<i>p</i> < 0.001). During the pandemic period, COI reductions were 32.3% in PAH and 93.5% in DC compared to usual care. Similar trends were observed in the post pandemic period, with COI reductions of 40.0% for PAH and 96.1% for DC.</p><p><strong>Conclusion: </strong>PAH and DC pathways did not worsen the clinical outcomes and reduced costs during and following the pandemic. As a result, these two pathways, developed during the COVID-19 pandemic, can be adapted for regular use. When these pathways are integrated into regular use, they can be promptly and fully reactivated in future emergencies.</p>","PeriodicalId":16740,"journal":{"name":"Journal of Pharmaceutical Policy and Practice","volume":"18 1","pages":"2544644"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392433/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of alternative care pathways adopted during the COVID-19 pandemic on the management of non-communicable diseases at a tertiary care hospital in Thailand.\",\"authors\":\"Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte\",\"doi\":\"10.1080/20523211.2025.2544644\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Management of non-communicable diseases (NCDs), including hypertension (HT) and diabetes mellitus (DM), was significantly impacted by the COVID-19 pandemic. Many institutions adopted alternative care pathways, e.g. pharmacy at home (PAH), and the deferred care (DC). While PAH has been studied for clinical outcomes, evaluation of the DC remains limited. Consequently, this study evaluates both the clinical and economic outcomes of the PAH and DC as alternatives to usual care.</p><p><strong>Method: </strong>A retrospective study was conducted at a tertiary care hospital in Thailand from 1 July 2021, to 30 June 2023. Data from outpatients with HT and DM were classified into PAH, DC, or discharged home with follow-up at the hospital. Clinical outcomes included changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), and fasting blood sugar (FBS), calculated from baseline to follow-up. Economic outcome was the cost of illness (COI) per patient visit. Multivariate multilevel mixed-effects linear regression assessed clinical outcomes, while log-linear regression evaluated economic outcome.</p><p><strong>Results: </strong>There were 3,518 patients in the pandemic period and 4,135 patients in the post pandemic period. There was no statistically significant impact of PAH and DC on changes in SBP, DBP, and FBS. However, both care pathways significantly reduced COI during both periods (<i>p</i> < 0.001). During the pandemic period, COI reductions were 32.3% in PAH and 93.5% in DC compared to usual care. Similar trends were observed in the post pandemic period, with COI reductions of 40.0% for PAH and 96.1% for DC.</p><p><strong>Conclusion: </strong>PAH and DC pathways did not worsen the clinical outcomes and reduced costs during and following the pandemic. As a result, these two pathways, developed during the COVID-19 pandemic, can be adapted for regular use. When these pathways are integrated into regular use, they can be promptly and fully reactivated in future emergencies.</p>\",\"PeriodicalId\":16740,\"journal\":{\"name\":\"Journal of Pharmaceutical Policy and Practice\",\"volume\":\"18 1\",\"pages\":\"2544644\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392433/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Policy and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20523211.2025.2544644\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20523211.2025.2544644","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
The impact of alternative care pathways adopted during the COVID-19 pandemic on the management of non-communicable diseases at a tertiary care hospital in Thailand.
Background: Management of non-communicable diseases (NCDs), including hypertension (HT) and diabetes mellitus (DM), was significantly impacted by the COVID-19 pandemic. Many institutions adopted alternative care pathways, e.g. pharmacy at home (PAH), and the deferred care (DC). While PAH has been studied for clinical outcomes, evaluation of the DC remains limited. Consequently, this study evaluates both the clinical and economic outcomes of the PAH and DC as alternatives to usual care.
Method: A retrospective study was conducted at a tertiary care hospital in Thailand from 1 July 2021, to 30 June 2023. Data from outpatients with HT and DM were classified into PAH, DC, or discharged home with follow-up at the hospital. Clinical outcomes included changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), and fasting blood sugar (FBS), calculated from baseline to follow-up. Economic outcome was the cost of illness (COI) per patient visit. Multivariate multilevel mixed-effects linear regression assessed clinical outcomes, while log-linear regression evaluated economic outcome.
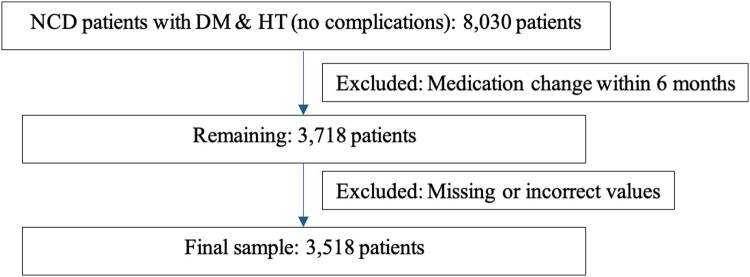
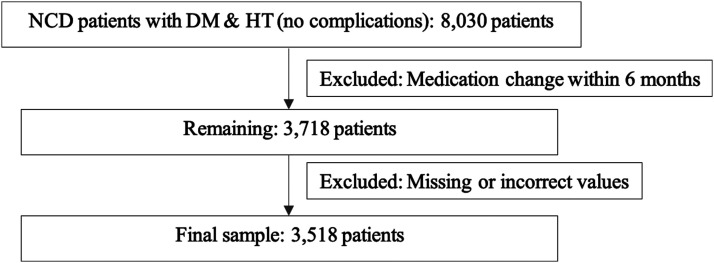
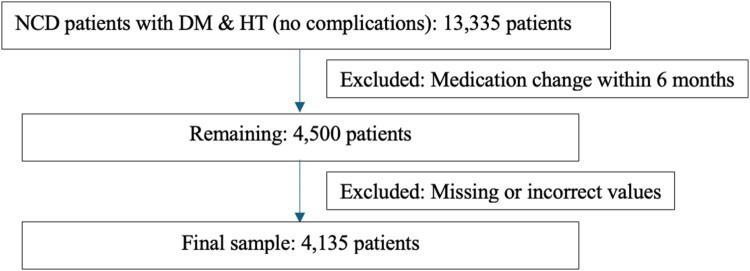
Results: There were 3,518 patients in the pandemic period and 4,135 patients in the post pandemic period. There was no statistically significant impact of PAH and DC on changes in SBP, DBP, and FBS. However, both care pathways significantly reduced COI during both periods (p < 0.001). During the pandemic period, COI reductions were 32.3% in PAH and 93.5% in DC compared to usual care. Similar trends were observed in the post pandemic period, with COI reductions of 40.0% for PAH and 96.1% for DC.
Conclusion: PAH and DC pathways did not worsen the clinical outcomes and reduced costs during and following the pandemic. As a result, these two pathways, developed during the COVID-19 pandemic, can be adapted for regular use. When these pathways are integrated into regular use, they can be promptly and fully reactivated in future emergencies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


