Francesco Del Giudice, Mohamed Gad, Valerio Santarelli, Rajesh Nair, Yasmin Abu-Ghanem, Elsie Mensah, Ben Challacombe, Jonathan Kam, Youssef Ibrahim, Basil Lufti, Amir Khan, Akra Yeasmin, Kathryn Chatterton, Suzanne Amery, Katarina Spurna, Romerr Alao, Syed Ghazi Ali Kirmani, Felice Crocetto, Biagio Barone, Bernardo Rocco, Alessandro Sciarra, Benjamin I Chung, Ramesh Thurairaja, Muhammad Shamim Khan
{"title":"迟发性和并发性膀胱切除术治疗行根治性膀胱切除术的非转移性尿路上皮癌:来自英国单一三级中心的围手术期和生存结果。","authors":"Francesco Del Giudice, Mohamed Gad, Valerio Santarelli, Rajesh Nair, Yasmin Abu-Ghanem, Elsie Mensah, Ben Challacombe, Jonathan Kam, Youssef Ibrahim, Basil Lufti, Amir Khan, Akra Yeasmin, Kathryn Chatterton, Suzanne Amery, Katarina Spurna, Romerr Alao, Syed Ghazi Ali Kirmani, Felice Crocetto, Biagio Barone, Bernardo Rocco, Alessandro Sciarra, Benjamin I Chung, Ramesh Thurairaja, Muhammad Shamim Khan","doi":"10.3390/jpm15080375","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> The role of urethrectomy at the time of Robotic-Assisted or Open Radical Cystectomy (RARC, ORC) is controversial. Whether urethrectomy should be performed at the time of RARC/ORC or delayed up to a 3-6 month interval is unclear. We performed a retrospective cohort analysis of perioperative and survival outcomes in patients with high-risk NMIBCs or non-metastatic MIBCs at our institution who underwent either concomitant or deferred urethrectomy after RC. <b>Materials and Methods:</b> cTis-T1 or cT2-T4, N0-1, M0 BC patients who underwent RARC or ORC from 2009 to 2024 were reviewed. Clinical, demographic, tumour, and patient characteristics and perioperative variables were assessed across concomitant and delayed urethrectomy groups. Multivariate logistic analysis was performed to estimate the impact of significant variables on intraoperative and postoperative outcomes. Univariable Kaplan-Meier and multivariable Cox regression modelling was implemented to explore the relative effect of time of urethrectomy on progression-free survival (PFS), cancer-specific survival (CSS), and overall survival (OS). <b>Results:</b> A total of <i>n</i> = 58 patients (<i>n</i> = 47 delayed vs. <i>n</i> = 11 concomitant) with similar demographic characteristics were included. The concomitant urethrectomy group experienced longer operative time and greater blood loss (379 ± 65 min and 430 ± 101 mL vs. 342 ± 82 min and 422 ± 125 mL, with <i>p</i> = 0.049 and <i>p</i> = 0.028, respectively). Hospital readmission rates were higher in the concomitant urethrectomy group (36.4% vs. 8.5%, <i>p</i> = 0.016; OR: 17.9; 95% CI 1.2-265; <i>p</i> = 0.036). In Cox regression analysis, the timing of urethrectomy had no influence on PFS, CSS, or OS (all <i>p</i> > 0.05). <b>Conclusions:</b> Our study suggests that urethrectomy can be safely deferred unless urothelial disease is clearly present pre- or intraoperatively without compromising survival outcome and with the advantage of reducing surgical morbidity at the time of RC.</p>","PeriodicalId":16722,"journal":{"name":"Journal of Personalized Medicine","volume":"15 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387265/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed vs. Concomitant Urethrectomy for Non-Metastatic Urothelial Carcinoma of the Urinary Bladder Undergoing Radical Cystectomy: Perioperative and Survival Outcomes from a Single Tertiary Centre in the United Kingdom.\",\"authors\":\"Francesco Del Giudice, Mohamed Gad, Valerio Santarelli, Rajesh Nair, Yasmin Abu-Ghanem, Elsie Mensah, Ben Challacombe, Jonathan Kam, Youssef Ibrahim, Basil Lufti, Amir Khan, Akra Yeasmin, Kathryn Chatterton, Suzanne Amery, Katarina Spurna, Romerr Alao, Syed Ghazi Ali Kirmani, Felice Crocetto, Biagio Barone, Bernardo Rocco, Alessandro Sciarra, Benjamin I Chung, Ramesh Thurairaja, Muhammad Shamim Khan\",\"doi\":\"10.3390/jpm15080375\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> The role of urethrectomy at the time of Robotic-Assisted or Open Radical Cystectomy (RARC, ORC) is controversial. Whether urethrectomy should be performed at the time of RARC/ORC or delayed up to a 3-6 month interval is unclear. We performed a retrospective cohort analysis of perioperative and survival outcomes in patients with high-risk NMIBCs or non-metastatic MIBCs at our institution who underwent either concomitant or deferred urethrectomy after RC. <b>Materials and Methods:</b> cTis-T1 or cT2-T4, N0-1, M0 BC patients who underwent RARC or ORC from 2009 to 2024 were reviewed. Clinical, demographic, tumour, and patient characteristics and perioperative variables were assessed across concomitant and delayed urethrectomy groups. Multivariate logistic analysis was performed to estimate the impact of significant variables on intraoperative and postoperative outcomes. Univariable Kaplan-Meier and multivariable Cox regression modelling was implemented to explore the relative effect of time of urethrectomy on progression-free survival (PFS), cancer-specific survival (CSS), and overall survival (OS). <b>Results:</b> A total of <i>n</i> = 58 patients (<i>n</i> = 47 delayed vs. <i>n</i> = 11 concomitant) with similar demographic characteristics were included. The concomitant urethrectomy group experienced longer operative time and greater blood loss (379 ± 65 min and 430 ± 101 mL vs. 342 ± 82 min and 422 ± 125 mL, with <i>p</i> = 0.049 and <i>p</i> = 0.028, respectively). Hospital readmission rates were higher in the concomitant urethrectomy group (36.4% vs. 8.5%, <i>p</i> = 0.016; OR: 17.9; 95% CI 1.2-265; <i>p</i> = 0.036). In Cox regression analysis, the timing of urethrectomy had no influence on PFS, CSS, or OS (all <i>p</i> > 0.05). <b>Conclusions:</b> Our study suggests that urethrectomy can be safely deferred unless urothelial disease is clearly present pre- or intraoperatively without compromising survival outcome and with the advantage of reducing surgical morbidity at the time of RC.</p>\",\"PeriodicalId\":16722,\"journal\":{\"name\":\"Journal of Personalized Medicine\",\"volume\":\"15 8\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387265/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Personalized Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jpm15080375\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jpm15080375","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
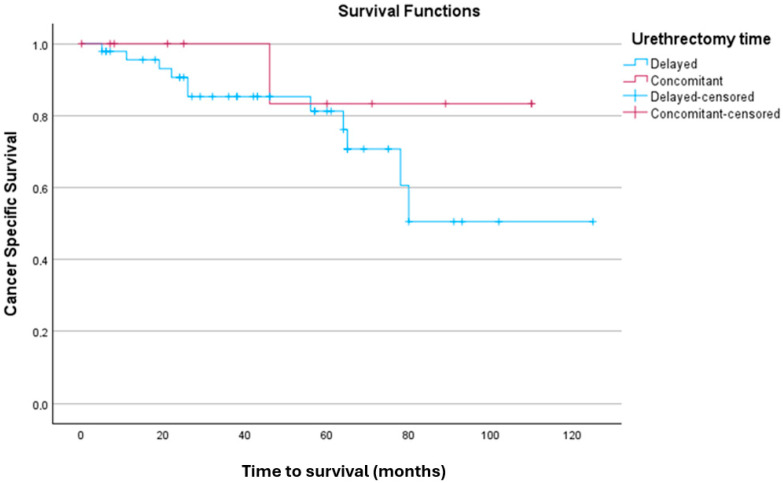
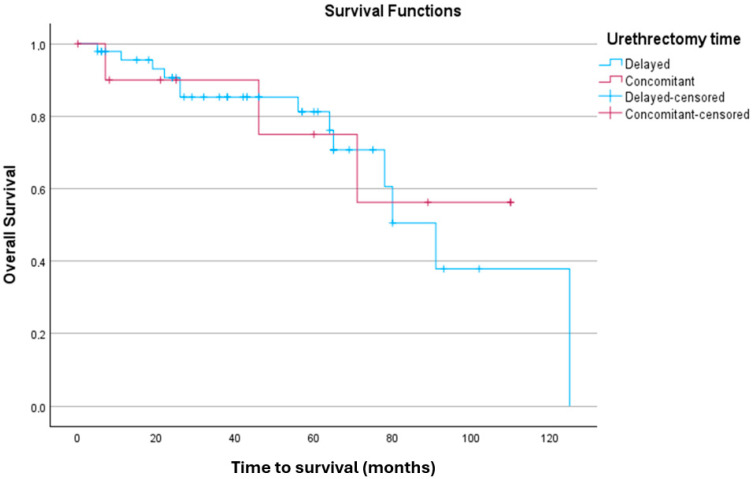
导读:在机器人辅助或开放式根治性膀胱切除术(RARC, ORC)中,尿道切除术的作用是有争议的。尿道切除术是否应该在RARC/ORC时进行,或延迟至3-6个月的间隔尚不清楚。我们进行了一项回顾性队列分析,分析了本院高危nmibc或非转移性mibc患者的围手术期和生存结果,这些患者在RC术后接受了合并或延期尿道切除术。材料与方法:回顾性分析2009 - 2024年接受RARC或ORC治疗的cTis-T1或cT2-T4、N0-1、M0例BC患者。临床、人口统计学、肿瘤、患者特征和围手术期变量对合并输尿管切除术组和延迟输尿管切除术组进行评估。采用多变量logistic分析来估计重要变量对术中及术后预后的影响。采用单变量Kaplan-Meier和多变量Cox回归模型,探讨输尿管切除术时间对无进展生存期(PFS)、癌症特异性生存期(CSS)和总生存期(OS)的相对影响。结果:共有n = 58例患者(n = 47延迟与n = 11伴随)具有相似的人口统计学特征。合并输尿管切除术组手术时间更长,出血量更大(379±65 min和430±101 mL vs. 342±82 min和422±125 mL, p = 0.049和p = 0.028)。合并输尿管切除术组再入院率较高(36.4%比8.5%,p = 0.016; OR: 17.9; 95% CI 1.2-265; p = 0.036)。在Cox回归分析中,输尿管切除术时间对PFS、CSS和OS无影响(均p < 0.05)。结论:我们的研究表明,除非术前或术中明确存在尿路上皮疾病,否则可以安全地推迟尿道切除术,而不会影响生存结果,并且具有减少RC时手术发病率的优势。
Delayed vs. Concomitant Urethrectomy for Non-Metastatic Urothelial Carcinoma of the Urinary Bladder Undergoing Radical Cystectomy: Perioperative and Survival Outcomes from a Single Tertiary Centre in the United Kingdom.
Introduction: The role of urethrectomy at the time of Robotic-Assisted or Open Radical Cystectomy (RARC, ORC) is controversial. Whether urethrectomy should be performed at the time of RARC/ORC or delayed up to a 3-6 month interval is unclear. We performed a retrospective cohort analysis of perioperative and survival outcomes in patients with high-risk NMIBCs or non-metastatic MIBCs at our institution who underwent either concomitant or deferred urethrectomy after RC. Materials and Methods: cTis-T1 or cT2-T4, N0-1, M0 BC patients who underwent RARC or ORC from 2009 to 2024 were reviewed. Clinical, demographic, tumour, and patient characteristics and perioperative variables were assessed across concomitant and delayed urethrectomy groups. Multivariate logistic analysis was performed to estimate the impact of significant variables on intraoperative and postoperative outcomes. Univariable Kaplan-Meier and multivariable Cox regression modelling was implemented to explore the relative effect of time of urethrectomy on progression-free survival (PFS), cancer-specific survival (CSS), and overall survival (OS). Results: A total of n = 58 patients (n = 47 delayed vs. n = 11 concomitant) with similar demographic characteristics were included. The concomitant urethrectomy group experienced longer operative time and greater blood loss (379 ± 65 min and 430 ± 101 mL vs. 342 ± 82 min and 422 ± 125 mL, with p = 0.049 and p = 0.028, respectively). Hospital readmission rates were higher in the concomitant urethrectomy group (36.4% vs. 8.5%, p = 0.016; OR: 17.9; 95% CI 1.2-265; p = 0.036). In Cox regression analysis, the timing of urethrectomy had no influence on PFS, CSS, or OS (all p > 0.05). Conclusions: Our study suggests that urethrectomy can be safely deferred unless urothelial disease is clearly present pre- or intraoperatively without compromising survival outcome and with the advantage of reducing surgical morbidity at the time of RC.
期刊介绍:
Journal of Personalized Medicine (JPM; ISSN 2075-4426) is an international, open access journal aimed at bringing all aspects of personalized medicine to one platform. JPM publishes cutting edge, innovative preclinical and translational scientific research and technologies related to personalized medicine (e.g., pharmacogenomics/proteomics, systems biology). JPM recognizes that personalized medicine—the assessment of genetic, environmental and host factors that cause variability of individuals—is a challenging, transdisciplinary topic that requires discussions from a range of experts. For a comprehensive perspective of personalized medicine, JPM aims to integrate expertise from the molecular and translational sciences, therapeutics and diagnostics, as well as discussions of regulatory, social, ethical and policy aspects. We provide a forum to bring together academic and clinical researchers, biotechnology, diagnostic and pharmaceutical companies, health professionals, regulatory and ethical experts, and government and regulatory authorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


