{"title":"在微创心脏手术中,正后方直径与从右小胸开路到正中胸骨开路的转换有关。","authors":"Quynh Nguyen, Durr Al-Hakim, Richard C Cook","doi":"10.3390/jpm15080353","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Minimally invasive cardiac surgery (MICS) via right minithoracotomy is a safe, reproducible approach with excellent outcomes and reduced costs compared to median sternotomy. Despite careful patient selection, conversion to sternotomy occurs in 1-3% of cases and is associated with significantly higher morbidity and mortality. Small body habitus, particularly a short anteroposterior (AP) diameter, may increase the risk of conversion, but this has not been previously studied. This study aims to identify preoperative factors associated with conversion to improve patient selection for MICS. As cardiovascular surgery becomes increasingly personalized, identifying anatomical factors that predict technical complexity is essential. <b>Methods</b>: This retrospective study included 254 adult patients who underwent elective MICS between 2015 and 2024 at a tertiary hospital. Patient characteristics, computed tomography (CT) scans, intraoperative parameters, and postoperative outcomes were reviewed. AP diameter was defined as the distance from the posterior sternum to the anterior vertebral body at the mitral valve level on CT. Statistical analyses included Mann-Whitney and Fisher's exact/chi-square tests. <b>Results</b>: Conversion to sternotomy occurred in 1.6% of patients (n = 4). All converted patients were female. The converted group had a significantly shorter median AP diameter (100 mm vs. 124 mm, <i>p</i> = 0.020). Conversion was associated with higher rates of stroke and infection (25.0% vs. 0.8%, <i>p</i> = 0.047 for both), but no significant differences in hospital stay, bleeding, or renal failure. <b>Conclusions:</b> An AP diameter of less than 100 mm was associated with a higher risk of conversion to sternotomy in MICS. Incorporating simple, reproducible preoperative imaging metrics into surgical planning may advance precision-guided cardiac surgery and optimize patient outcomes.</p>","PeriodicalId":16722,"journal":{"name":"Journal of Personalized Medicine","volume":"15 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387597/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anteroposterior Diameter Is Associated with Conversion from Right Minithoracotomy to Median Sternotomy in Minimally Invasive Cardiac Surgery.\",\"authors\":\"Quynh Nguyen, Durr Al-Hakim, Richard C Cook\",\"doi\":\"10.3390/jpm15080353\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b>: Minimally invasive cardiac surgery (MICS) via right minithoracotomy is a safe, reproducible approach with excellent outcomes and reduced costs compared to median sternotomy. Despite careful patient selection, conversion to sternotomy occurs in 1-3% of cases and is associated with significantly higher morbidity and mortality. Small body habitus, particularly a short anteroposterior (AP) diameter, may increase the risk of conversion, but this has not been previously studied. This study aims to identify preoperative factors associated with conversion to improve patient selection for MICS. As cardiovascular surgery becomes increasingly personalized, identifying anatomical factors that predict technical complexity is essential. <b>Methods</b>: This retrospective study included 254 adult patients who underwent elective MICS between 2015 and 2024 at a tertiary hospital. Patient characteristics, computed tomography (CT) scans, intraoperative parameters, and postoperative outcomes were reviewed. AP diameter was defined as the distance from the posterior sternum to the anterior vertebral body at the mitral valve level on CT. Statistical analyses included Mann-Whitney and Fisher's exact/chi-square tests. <b>Results</b>: Conversion to sternotomy occurred in 1.6% of patients (n = 4). All converted patients were female. The converted group had a significantly shorter median AP diameter (100 mm vs. 124 mm, <i>p</i> = 0.020). Conversion was associated with higher rates of stroke and infection (25.0% vs. 0.8%, <i>p</i> = 0.047 for both), but no significant differences in hospital stay, bleeding, or renal failure. <b>Conclusions:</b> An AP diameter of less than 100 mm was associated with a higher risk of conversion to sternotomy in MICS. Incorporating simple, reproducible preoperative imaging metrics into surgical planning may advance precision-guided cardiac surgery and optimize patient outcomes.</p>\",\"PeriodicalId\":16722,\"journal\":{\"name\":\"Journal of Personalized Medicine\",\"volume\":\"15 8\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387597/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Personalized Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jpm15080353\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jpm15080353","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
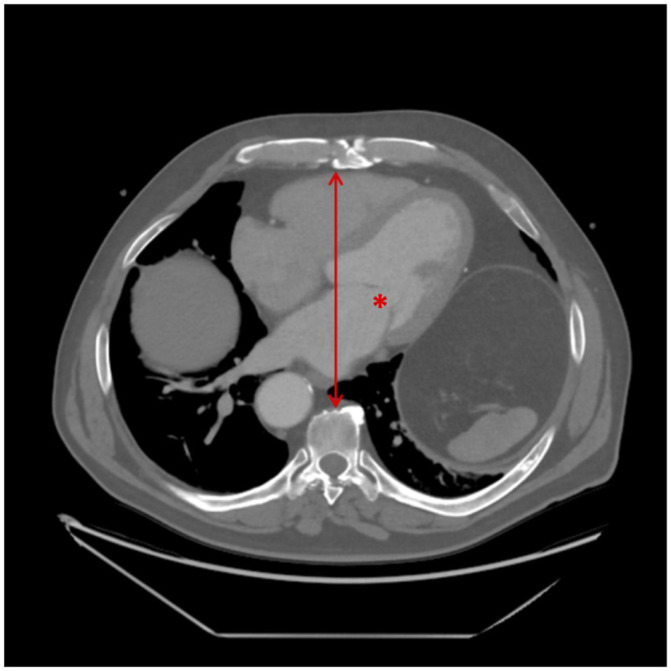
背景:与胸骨正中切开术相比,经右小胸切开术的微创心脏手术是一种安全、可重复的方法,具有良好的疗效和较低的成本。尽管谨慎选择患者,但转换为胸骨切开术的病例发生率为1-3%,并伴有较高的发病率和死亡率。体型小,尤其是前后径短,可能会增加转体的风险,但这一点以前没有研究过。本研究旨在确定术前与转换相关的因素,以改善MICS患者的选择。随着心血管手术变得越来越个性化,确定预测技术复杂性的解剖学因素至关重要。方法:本回顾性研究纳入了2015年至2024年在某三级医院接受选择性MICS的254例成年患者。回顾了患者特征、计算机断层扫描(CT)、术中参数和术后结果。AP直径定义为CT上胸骨后部到前椎体在二尖瓣水平处的距离。统计分析包括Mann-Whitney和Fisher的精确/卡方检验。结果:1.6%的患者进行了胸骨切开术(n = 4)。所有转化患者均为女性。转换组的中位AP直径显著缩短(100 mm比124 mm, p = 0.020)。转换与较高的卒中和感染发生率相关(25.0%对0.8%,两者p = 0.047),但在住院时间、出血或肾衰竭方面无显著差异。结论:在MICS患者中,AP直径小于100mm与胸骨切开术转换的高风险相关。将简单的、可重复的术前成像指标纳入手术计划,可以推进精确指导的心脏手术,并优化患者的预后。
Anteroposterior Diameter Is Associated with Conversion from Right Minithoracotomy to Median Sternotomy in Minimally Invasive Cardiac Surgery.
Background: Minimally invasive cardiac surgery (MICS) via right minithoracotomy is a safe, reproducible approach with excellent outcomes and reduced costs compared to median sternotomy. Despite careful patient selection, conversion to sternotomy occurs in 1-3% of cases and is associated with significantly higher morbidity and mortality. Small body habitus, particularly a short anteroposterior (AP) diameter, may increase the risk of conversion, but this has not been previously studied. This study aims to identify preoperative factors associated with conversion to improve patient selection for MICS. As cardiovascular surgery becomes increasingly personalized, identifying anatomical factors that predict technical complexity is essential. Methods: This retrospective study included 254 adult patients who underwent elective MICS between 2015 and 2024 at a tertiary hospital. Patient characteristics, computed tomography (CT) scans, intraoperative parameters, and postoperative outcomes were reviewed. AP diameter was defined as the distance from the posterior sternum to the anterior vertebral body at the mitral valve level on CT. Statistical analyses included Mann-Whitney and Fisher's exact/chi-square tests. Results: Conversion to sternotomy occurred in 1.6% of patients (n = 4). All converted patients were female. The converted group had a significantly shorter median AP diameter (100 mm vs. 124 mm, p = 0.020). Conversion was associated with higher rates of stroke and infection (25.0% vs. 0.8%, p = 0.047 for both), but no significant differences in hospital stay, bleeding, or renal failure. Conclusions: An AP diameter of less than 100 mm was associated with a higher risk of conversion to sternotomy in MICS. Incorporating simple, reproducible preoperative imaging metrics into surgical planning may advance precision-guided cardiac surgery and optimize patient outcomes.
期刊介绍:
Journal of Personalized Medicine (JPM; ISSN 2075-4426) is an international, open access journal aimed at bringing all aspects of personalized medicine to one platform. JPM publishes cutting edge, innovative preclinical and translational scientific research and technologies related to personalized medicine (e.g., pharmacogenomics/proteomics, systems biology). JPM recognizes that personalized medicine—the assessment of genetic, environmental and host factors that cause variability of individuals—is a challenging, transdisciplinary topic that requires discussions from a range of experts. For a comprehensive perspective of personalized medicine, JPM aims to integrate expertise from the molecular and translational sciences, therapeutics and diagnostics, as well as discussions of regulatory, social, ethical and policy aspects. We provide a forum to bring together academic and clinical researchers, biotechnology, diagnostic and pharmaceutical companies, health professionals, regulatory and ethical experts, and government and regulatory authorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


