{"title":"骨质疏松性椎体压缩性骨折的最佳治疗:网络荟萃分析。","authors":"Yan Li, Xianghong Wang, Jianfeng Sun, Maozhen Ma","doi":"10.1186/s13018-025-06233-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Optimal management of osteoporotic vertebral compression fractures (OVCFs) remains controversial. This network meta‑analysis (NMA) evaluated the relative efficacy and safety of third‑generation percutaneous vertebral augmentation (TVA), percutaneous kyphoplasty (PKP), percutaneous vertebroplasty (PVP), and non‑surgical management (NSM) in OVCFs.</p><p><strong>Methods: </strong>A systematic search of PubMed, Embase, the Cochrane Library, and Web of Science was conducted from inception to February 1, 2025, to identify clinical trials comparing ≥ 2 of these interventions. Primary outcomes included pain intensity (Visual Analog Scale [VAS]), functional disability (Oswestry Disability Index [ODI]), quality of life (EQ‑5D), and anterior vertebral body height (AVB). Adverse events, including adjacent vertebral fracture (AVF) and bone cement leakage (BCL), were also assessed.</p><p><strong>Results: </strong>Forty‑six studies (23 RCTs and 23 comparative cohort studies; n = 5,660) were included. Both TVA and PKP yielded greater VAS reductions than NSM at short‑term (≤ 6 months; MD - 1.28 and - 1.37; 95% CI - 1.62 to - 0.93 and - 1.82 to - 0.92) and long‑term (> 6 months; MD - 0.86 and - 0.69; 95% CI - 1.22 to - 0.50 and - 1.20 to - 0.19) follow‑up. TVA outperformed NSM in ODI improvement at short‑term (MD - 6.84; 95% CI - 9.84 to - 3.84) and long‑term (MD - 9.14; 95% CI - 14.64 to - 3.65); PKP surpassed NSM short‑term (MD - 5.59; 95% CI - 9.32 to - 1.86) but was inferior to TVA long‑term (MD 8.34; 95% CI 2.62 to 14.06). Surgical interventions uniformly outperformed NSM in quality‑of‑life gains. TVA and PKP achieved greater AVB restoration than NSM, whereas PVP carried a higher BCL risk compared to TVA and PKP. NSM was associated with the lowest probability of AVF (90.2%).</p><p><strong>Conclusions: </strong>Although PKP offers the greatest long‑term preservation of AVB, third‑generation TVA appears superior to PVP, PKP, and NSM in improving pain, functional disability, quality of life, and safety in OVCF patients. High‑quality randomized trials with extended follow‑up are required to confirm these findings.</p>","PeriodicalId":16629,"journal":{"name":"Journal of Orthopaedic Surgery and Research","volume":"20 1","pages":"810"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398152/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimal management for osteoporotic vertebral compression fractures: a network meta-analysis.\",\"authors\":\"Yan Li, Xianghong Wang, Jianfeng Sun, Maozhen Ma\",\"doi\":\"10.1186/s13018-025-06233-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Optimal management of osteoporotic vertebral compression fractures (OVCFs) remains controversial. This network meta‑analysis (NMA) evaluated the relative efficacy and safety of third‑generation percutaneous vertebral augmentation (TVA), percutaneous kyphoplasty (PKP), percutaneous vertebroplasty (PVP), and non‑surgical management (NSM) in OVCFs.</p><p><strong>Methods: </strong>A systematic search of PubMed, Embase, the Cochrane Library, and Web of Science was conducted from inception to February 1, 2025, to identify clinical trials comparing ≥ 2 of these interventions. Primary outcomes included pain intensity (Visual Analog Scale [VAS]), functional disability (Oswestry Disability Index [ODI]), quality of life (EQ‑5D), and anterior vertebral body height (AVB). Adverse events, including adjacent vertebral fracture (AVF) and bone cement leakage (BCL), were also assessed.</p><p><strong>Results: </strong>Forty‑six studies (23 RCTs and 23 comparative cohort studies; n = 5,660) were included. Both TVA and PKP yielded greater VAS reductions than NSM at short‑term (≤ 6 months; MD - 1.28 and - 1.37; 95% CI - 1.62 to - 0.93 and - 1.82 to - 0.92) and long‑term (> 6 months; MD - 0.86 and - 0.69; 95% CI - 1.22 to - 0.50 and - 1.20 to - 0.19) follow‑up. TVA outperformed NSM in ODI improvement at short‑term (MD - 6.84; 95% CI - 9.84 to - 3.84) and long‑term (MD - 9.14; 95% CI - 14.64 to - 3.65); PKP surpassed NSM short‑term (MD - 5.59; 95% CI - 9.32 to - 1.86) but was inferior to TVA long‑term (MD 8.34; 95% CI 2.62 to 14.06). Surgical interventions uniformly outperformed NSM in quality‑of‑life gains. TVA and PKP achieved greater AVB restoration than NSM, whereas PVP carried a higher BCL risk compared to TVA and PKP. NSM was associated with the lowest probability of AVF (90.2%).</p><p><strong>Conclusions: </strong>Although PKP offers the greatest long‑term preservation of AVB, third‑generation TVA appears superior to PVP, PKP, and NSM in improving pain, functional disability, quality of life, and safety in OVCF patients. High‑quality randomized trials with extended follow‑up are required to confirm these findings.</p>\",\"PeriodicalId\":16629,\"journal\":{\"name\":\"Journal of Orthopaedic Surgery and Research\",\"volume\":\"20 1\",\"pages\":\"810\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398152/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Orthopaedic Surgery and Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13018-025-06233-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Surgery and Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13018-025-06233-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
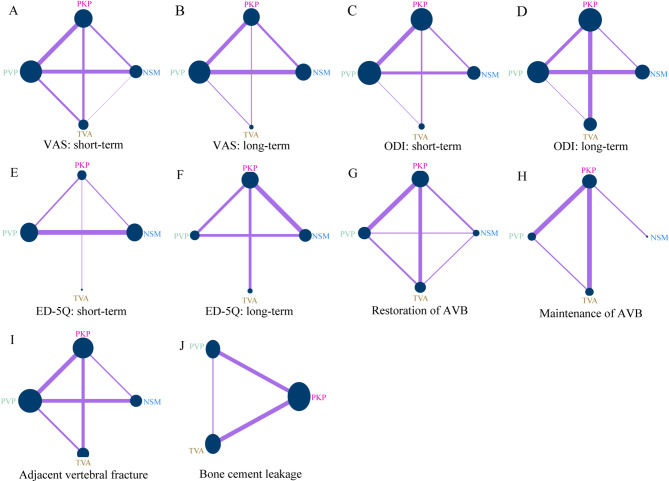
背景:骨质疏松性椎体压缩性骨折(OVCFs)的最佳治疗仍然存在争议。该网络荟萃分析(NMA)评估了第三代经皮椎体增强术(TVA)、经皮椎体后凸成形术(PKP)、经皮椎体成形术(PVP)和非手术治疗(NSM)治疗ovcf的相对疗效和安全性。方法:系统检索PubMed、Embase、Cochrane图书馆和Web of Science,从研究开始到2025年2月1日,确定比较≥2种干预措施的临床试验。主要结局包括疼痛强度(视觉模拟量表[VAS])、功能残疾(Oswestry残疾指数[ODI])、生活质量(EQ - 5D)和前椎体高度(AVB)。不良事件,包括相邻椎体骨折(AVF)和骨水泥渗漏(BCL),也进行了评估。结果:纳入46项研究(23项随机对照试验和23项比较队列研究,n = 5,660)。TVA和PKP在短期(≤6个月;MD - 1.28和- 1.37;95% CI - 1.62至- 0.93和- 1.82至- 0.92)和长期(bbb6个月;MD - 0.86和- 0.69;95% CI - 1.22至- 0.50和- 1.20至- 0.19)随访中均比NSM产生更大的VAS降低。TVA在短期(MD - 6.84; 95% CI - 9.84至- 3.84)和长期(MD - 9.14; 95% CI - 14.64至- 3.65)改善ODI方面优于NSM;PKP短期优于NSM (MD - 5.59; 95% CI - 9.32至- 1.86),但长期优于TVA (MD 8.34; 95% CI 2.62至14.06)。在生活质量方面,手术干预均优于NSM。TVA和PKP比NSM更能恢复AVB,而PVP比TVA和PKP有更高的BCL风险。NSM与AVF发生率最低(90.2%)相关。结论:尽管PKP提供了最大的AVB长期保存,第三代TVA在改善OVCF患者的疼痛、功能残疾、生活质量和安全性方面优于PVP、PKP和NSM。需要高质量的随机试验和长期随访来证实这些发现。
Optimal management for osteoporotic vertebral compression fractures: a network meta-analysis.
Background: Optimal management of osteoporotic vertebral compression fractures (OVCFs) remains controversial. This network meta‑analysis (NMA) evaluated the relative efficacy and safety of third‑generation percutaneous vertebral augmentation (TVA), percutaneous kyphoplasty (PKP), percutaneous vertebroplasty (PVP), and non‑surgical management (NSM) in OVCFs.
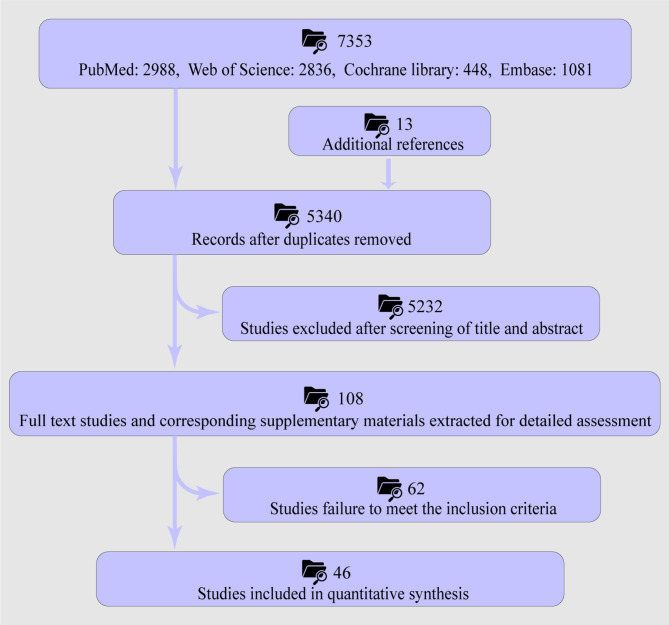
Methods: A systematic search of PubMed, Embase, the Cochrane Library, and Web of Science was conducted from inception to February 1, 2025, to identify clinical trials comparing ≥ 2 of these interventions. Primary outcomes included pain intensity (Visual Analog Scale [VAS]), functional disability (Oswestry Disability Index [ODI]), quality of life (EQ‑5D), and anterior vertebral body height (AVB). Adverse events, including adjacent vertebral fracture (AVF) and bone cement leakage (BCL), were also assessed.
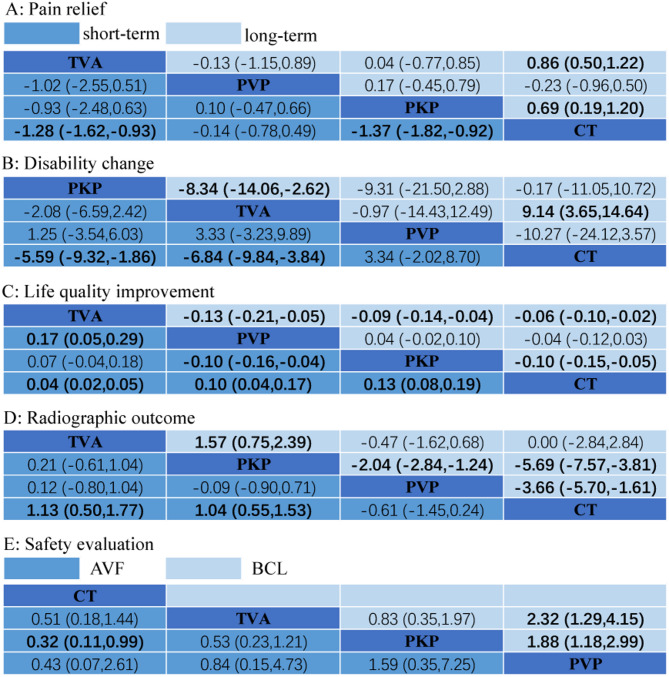
Results: Forty‑six studies (23 RCTs and 23 comparative cohort studies; n = 5,660) were included. Both TVA and PKP yielded greater VAS reductions than NSM at short‑term (≤ 6 months; MD - 1.28 and - 1.37; 95% CI - 1.62 to - 0.93 and - 1.82 to - 0.92) and long‑term (> 6 months; MD - 0.86 and - 0.69; 95% CI - 1.22 to - 0.50 and - 1.20 to - 0.19) follow‑up. TVA outperformed NSM in ODI improvement at short‑term (MD - 6.84; 95% CI - 9.84 to - 3.84) and long‑term (MD - 9.14; 95% CI - 14.64 to - 3.65); PKP surpassed NSM short‑term (MD - 5.59; 95% CI - 9.32 to - 1.86) but was inferior to TVA long‑term (MD 8.34; 95% CI 2.62 to 14.06). Surgical interventions uniformly outperformed NSM in quality‑of‑life gains. TVA and PKP achieved greater AVB restoration than NSM, whereas PVP carried a higher BCL risk compared to TVA and PKP. NSM was associated with the lowest probability of AVF (90.2%).
Conclusions: Although PKP offers the greatest long‑term preservation of AVB, third‑generation TVA appears superior to PVP, PKP, and NSM in improving pain, functional disability, quality of life, and safety in OVCF patients. High‑quality randomized trials with extended follow‑up are required to confirm these findings.
期刊介绍:
Journal of Orthopaedic Surgery and Research is an open access journal that encompasses all aspects of clinical and basic research studies related to musculoskeletal issues.
Orthopaedic research is conducted at clinical and basic science levels. With the advancement of new technologies and the increasing expectation and demand from doctors and patients, we are witnessing an enormous growth in clinical orthopaedic research, particularly in the fields of traumatology, spinal surgery, joint replacement, sports medicine, musculoskeletal tumour management, hand microsurgery, foot and ankle surgery, paediatric orthopaedic, and orthopaedic rehabilitation. The involvement of basic science ranges from molecular, cellular, structural and functional perspectives to tissue engineering, gait analysis, automation and robotic surgery. Implant and biomaterial designs are new disciplines that complement clinical applications.
JOSR encourages the publication of multidisciplinary research with collaboration amongst clinicians and scientists from different disciplines, which will be the trend in the coming decades.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


