Melih Z Kaya, Pradeep Banerjee, Cenk Ayata, Andrea M Harriott
{"title":"口服抗炎剂减轻小鼠去极化引起的疼痛和焦虑行为。","authors":"Melih Z Kaya, Pradeep Banerjee, Cenk Ayata, Andrea M Harriott","doi":"10.1186/s10194-025-02125-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spreading depolarization (SD) is the most likely cause of migraine aura and may be linked to trigeminal nociception. Using minimally invasive optogenetic SD induction (opto-SD), we previously showed that SD triggers acute periorbital mechanical allodynia-like behavior, supporting SD-induced activation of migraine-relevant trigeminal pain pathways. Here, we tested whether selective oral calcitonin gene-related peptide (CGRP) receptor antagonist, atogepant, could ameliorate SD-evoked pain and anxiety phenotypes.</p><p><strong>Methods: </strong>Thirty-two adult male and female Thy1-ChR2-EYFP transgenic mice (3-5 months, 18-30 g) housed in 12/12-hr light/dark cycles were used. Under brief isoflurane anesthesia, a thin glass panel was placed on intact skull one week before the experiment to achieve translucency. A single SD was evoked using 10 s, 10 mW blue light stimulation over the motor cortex. One hour before SD or sham stimulation, atogepant (ato; 30 mg/kg in 100% PEG400) or vehicle (veh; 100% PEG400) was administered by oral gavage (4 mL/kg). Mechanical periorbital thresholds were measured 1 h after SD using von Frey monofilaments. Mouse grimace was then quantified using PainFace, an open convolutional neural network platform. Lastly, anxiety-like behavior was examined in an open field. Groups were randomly assigned and the investigator blinded to group allocation (n = 8/group, balanced by sex), p < 0.05 was considered significant.</p><p><strong>Results: </strong>There was a significant main effect of SD (p < 0.001) and atogepant (p = 0.015) on the periorbital threshold with an interaction (p < 0.001). A single opto-SD lowered periorbital threshold compared with sham (veh sham vs. veh SD: p < 0.001). SD also increased the total grimace score compared with sham (veh sham vs. veh SD: p = 0.014). Oral atogepant (30 mg/kg) alleviated SD-induced periorbital allodynia-like behavior (veh SD vs. ato SD: p < 0.001) but did not completely reverse SD-induced periorbital allodynia-like behavior (ato sham vs. ato SD: p < 0.001). Atogepant abolished the SD-induced facial grimace (ato sham vs. ato SD: p = 0.238). SD increased thigmotaxis score compared with sham (veh sham vs. veh SD: p = 0.016). Following atogepant treatment, there was no difference in thigmotaxis score in SD versus sham groups (ato sham vs. ato SD: p = 0.200).</p><p><strong>Conclusions: </strong>These data suggest SD provokes a reproducible and robust facial pain phenotype in mice that is alleviated by pre-administration with atogepant. There was also improvement in SD-induced anxiety-like behavior following atogepant.</p>","PeriodicalId":16013,"journal":{"name":"Journal of Headache and Pain","volume":"26 1","pages":"187"},"PeriodicalIF":7.9000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12369159/pdf/","citationCount":"0","resultStr":"{\"title\":\"Oral atogepant mitigates spreading depolarization-induced pain and anxiety behavior in mice.\",\"authors\":\"Melih Z Kaya, Pradeep Banerjee, Cenk Ayata, Andrea M Harriott\",\"doi\":\"10.1186/s10194-025-02125-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Spreading depolarization (SD) is the most likely cause of migraine aura and may be linked to trigeminal nociception. Using minimally invasive optogenetic SD induction (opto-SD), we previously showed that SD triggers acute periorbital mechanical allodynia-like behavior, supporting SD-induced activation of migraine-relevant trigeminal pain pathways. Here, we tested whether selective oral calcitonin gene-related peptide (CGRP) receptor antagonist, atogepant, could ameliorate SD-evoked pain and anxiety phenotypes.</p><p><strong>Methods: </strong>Thirty-two adult male and female Thy1-ChR2-EYFP transgenic mice (3-5 months, 18-30 g) housed in 12/12-hr light/dark cycles were used. Under brief isoflurane anesthesia, a thin glass panel was placed on intact skull one week before the experiment to achieve translucency. A single SD was evoked using 10 s, 10 mW blue light stimulation over the motor cortex. One hour before SD or sham stimulation, atogepant (ato; 30 mg/kg in 100% PEG400) or vehicle (veh; 100% PEG400) was administered by oral gavage (4 mL/kg). Mechanical periorbital thresholds were measured 1 h after SD using von Frey monofilaments. Mouse grimace was then quantified using PainFace, an open convolutional neural network platform. Lastly, anxiety-like behavior was examined in an open field. Groups were randomly assigned and the investigator blinded to group allocation (n = 8/group, balanced by sex), p < 0.05 was considered significant.</p><p><strong>Results: </strong>There was a significant main effect of SD (p < 0.001) and atogepant (p = 0.015) on the periorbital threshold with an interaction (p < 0.001). A single opto-SD lowered periorbital threshold compared with sham (veh sham vs. veh SD: p < 0.001). SD also increased the total grimace score compared with sham (veh sham vs. veh SD: p = 0.014). Oral atogepant (30 mg/kg) alleviated SD-induced periorbital allodynia-like behavior (veh SD vs. ato SD: p < 0.001) but did not completely reverse SD-induced periorbital allodynia-like behavior (ato sham vs. ato SD: p < 0.001). Atogepant abolished the SD-induced facial grimace (ato sham vs. ato SD: p = 0.238). SD increased thigmotaxis score compared with sham (veh sham vs. veh SD: p = 0.016). Following atogepant treatment, there was no difference in thigmotaxis score in SD versus sham groups (ato sham vs. ato SD: p = 0.200).</p><p><strong>Conclusions: </strong>These data suggest SD provokes a reproducible and robust facial pain phenotype in mice that is alleviated by pre-administration with atogepant. There was also improvement in SD-induced anxiety-like behavior following atogepant.</p>\",\"PeriodicalId\":16013,\"journal\":{\"name\":\"Journal of Headache and Pain\",\"volume\":\"26 1\",\"pages\":\"187\"},\"PeriodicalIF\":7.9000,\"publicationDate\":\"2025-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12369159/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Headache and Pain\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s10194-025-02125-w\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Headache and Pain","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10194-025-02125-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Oral atogepant mitigates spreading depolarization-induced pain and anxiety behavior in mice.
Background: Spreading depolarization (SD) is the most likely cause of migraine aura and may be linked to trigeminal nociception. Using minimally invasive optogenetic SD induction (opto-SD), we previously showed that SD triggers acute periorbital mechanical allodynia-like behavior, supporting SD-induced activation of migraine-relevant trigeminal pain pathways. Here, we tested whether selective oral calcitonin gene-related peptide (CGRP) receptor antagonist, atogepant, could ameliorate SD-evoked pain and anxiety phenotypes.
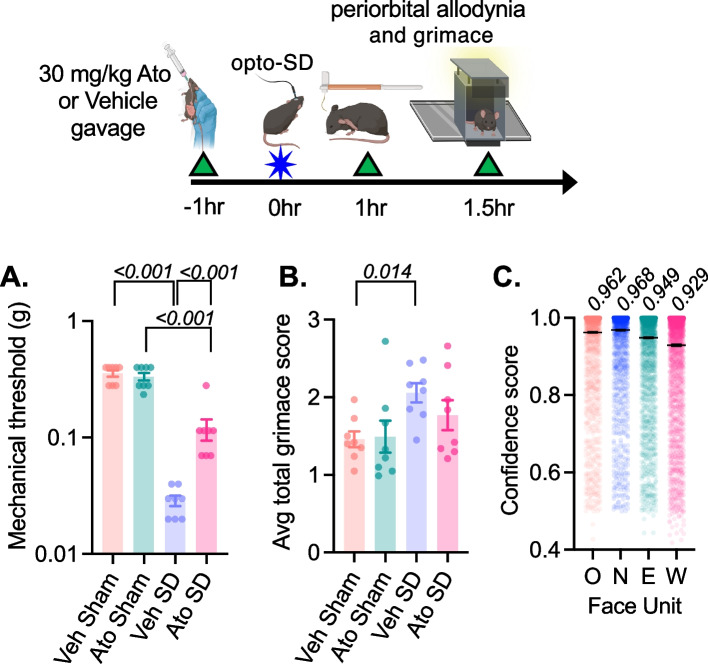
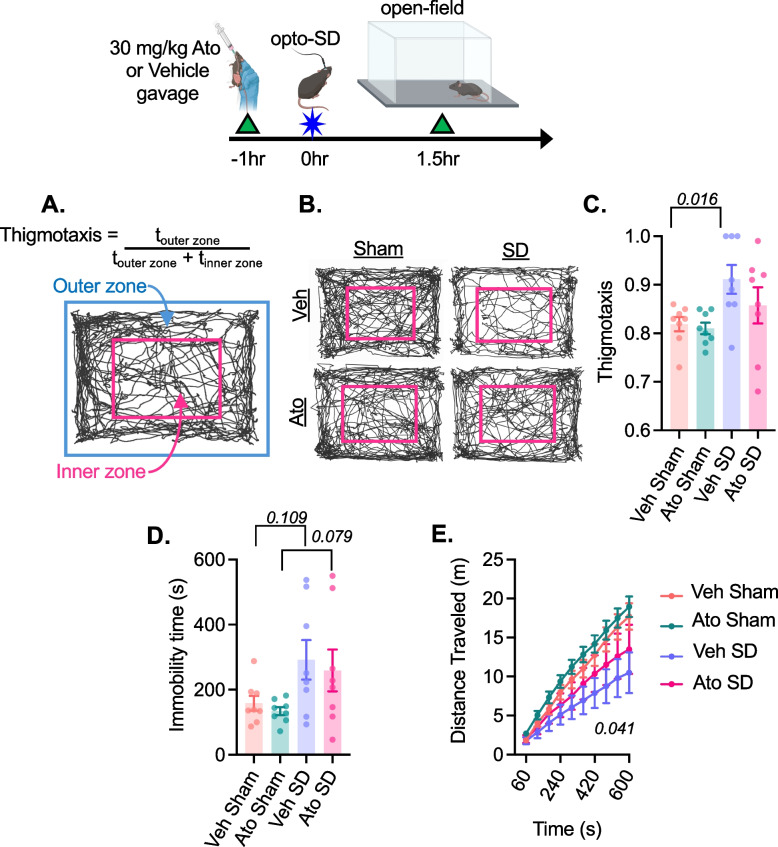
Methods: Thirty-two adult male and female Thy1-ChR2-EYFP transgenic mice (3-5 months, 18-30 g) housed in 12/12-hr light/dark cycles were used. Under brief isoflurane anesthesia, a thin glass panel was placed on intact skull one week before the experiment to achieve translucency. A single SD was evoked using 10 s, 10 mW blue light stimulation over the motor cortex. One hour before SD or sham stimulation, atogepant (ato; 30 mg/kg in 100% PEG400) or vehicle (veh; 100% PEG400) was administered by oral gavage (4 mL/kg). Mechanical periorbital thresholds were measured 1 h after SD using von Frey monofilaments. Mouse grimace was then quantified using PainFace, an open convolutional neural network platform. Lastly, anxiety-like behavior was examined in an open field. Groups were randomly assigned and the investigator blinded to group allocation (n = 8/group, balanced by sex), p < 0.05 was considered significant.
Results: There was a significant main effect of SD (p < 0.001) and atogepant (p = 0.015) on the periorbital threshold with an interaction (p < 0.001). A single opto-SD lowered periorbital threshold compared with sham (veh sham vs. veh SD: p < 0.001). SD also increased the total grimace score compared with sham (veh sham vs. veh SD: p = 0.014). Oral atogepant (30 mg/kg) alleviated SD-induced periorbital allodynia-like behavior (veh SD vs. ato SD: p < 0.001) but did not completely reverse SD-induced periorbital allodynia-like behavior (ato sham vs. ato SD: p < 0.001). Atogepant abolished the SD-induced facial grimace (ato sham vs. ato SD: p = 0.238). SD increased thigmotaxis score compared with sham (veh sham vs. veh SD: p = 0.016). Following atogepant treatment, there was no difference in thigmotaxis score in SD versus sham groups (ato sham vs. ato SD: p = 0.200).
Conclusions: These data suggest SD provokes a reproducible and robust facial pain phenotype in mice that is alleviated by pre-administration with atogepant. There was also improvement in SD-induced anxiety-like behavior following atogepant.
期刊介绍:
The Journal of Headache and Pain, a peer-reviewed open-access journal published under the BMC brand, a part of Springer Nature, is dedicated to researchers engaged in all facets of headache and related pain syndromes. It encompasses epidemiology, public health, basic science, translational medicine, clinical trials, and real-world data.
With a multidisciplinary approach, The Journal of Headache and Pain addresses headache medicine and related pain syndromes across all medical disciplines. It particularly encourages submissions in clinical, translational, and basic science fields, focusing on pain management, genetics, neurology, and internal medicine. The journal publishes research articles, reviews, letters to the Editor, as well as consensus articles and guidelines, aimed at promoting best practices in managing patients with headaches and related pain.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


