{"title":"南非约翰内斯堡st段抬高型心肌梗死30天和1年全因死亡率:来自STEMI HOC-1前瞻性研究的见解","authors":"Marheb Badianyama, Arthur Mutyaba, Nqoba Tsabedze","doi":"10.3390/jcdd12080282","DOIUrl":null,"url":null,"abstract":"<p><p>Despite the increased mortality due to ST-segment elevation myocardial infarction (STEMI) in South Africa (SA), SA lacks comprehensive data on STEMI clinical outcomes. This study aimed to determine the 30-day and one-year all-cause mortality rates of STEMI patients presenting to our hospital. This was a one-year prospective single-centre study of STEMI patients presenting to the Charlotte Maxeke Johannesburg Hospital in SA between December 2021 and August 2023. We compared the baseline clinical characteristics, reperfusion strategies, and in-hospital, 30-day, and one-year clinical outcomes of survivors and non-survivors. This cohort included 378 STEMI participants. The in-hospital, 30-day, and one-year all-cause mortality rates were 6.6% (n = 25), 10.1% (n = 38), and 17.2% (n = 65), respectively. The pharmacoinvasive strategy was the most used reperfusion therapy (n = 150, 39.7%). On adjusted multivariate Cox regression analysis, a Killip class >2 was the strongest independent predictor of 30-day [HR 5.61, 95% CI 2.83-11.12; <i>p</i> < 0.001] and one-year all-cause mortality [HR 1.72, 95% CI 1.26-2.34; <i>p</i> = 0.001]. Although mortality has increased, our mortality rates were comparable to outcomes from high-income countries but significantly lower than reports from other low- or middle-income countries. Importantly, there were no significant differences in 30-day and one-year survival outcomes between the different reperfusion strategies.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387001/pdf/","citationCount":"0","resultStr":"{\"title\":\"Thirty-Day and One-Year All-Cause Mortality of ST-Segment Elevation Myocardial Infarction in Johannesburg, South Africa: Insights from the STEMI HOC-1 Prospective Study.\",\"authors\":\"Marheb Badianyama, Arthur Mutyaba, Nqoba Tsabedze\",\"doi\":\"10.3390/jcdd12080282\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Despite the increased mortality due to ST-segment elevation myocardial infarction (STEMI) in South Africa (SA), SA lacks comprehensive data on STEMI clinical outcomes. This study aimed to determine the 30-day and one-year all-cause mortality rates of STEMI patients presenting to our hospital. This was a one-year prospective single-centre study of STEMI patients presenting to the Charlotte Maxeke Johannesburg Hospital in SA between December 2021 and August 2023. We compared the baseline clinical characteristics, reperfusion strategies, and in-hospital, 30-day, and one-year clinical outcomes of survivors and non-survivors. This cohort included 378 STEMI participants. The in-hospital, 30-day, and one-year all-cause mortality rates were 6.6% (n = 25), 10.1% (n = 38), and 17.2% (n = 65), respectively. The pharmacoinvasive strategy was the most used reperfusion therapy (n = 150, 39.7%). On adjusted multivariate Cox regression analysis, a Killip class >2 was the strongest independent predictor of 30-day [HR 5.61, 95% CI 2.83-11.12; <i>p</i> < 0.001] and one-year all-cause mortality [HR 1.72, 95% CI 1.26-2.34; <i>p</i> = 0.001]. Although mortality has increased, our mortality rates were comparable to outcomes from high-income countries but significantly lower than reports from other low- or middle-income countries. Importantly, there were no significant differences in 30-day and one-year survival outcomes between the different reperfusion strategies.</p>\",\"PeriodicalId\":15197,\"journal\":{\"name\":\"Journal of Cardiovascular Development and Disease\",\"volume\":\"12 8\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387001/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Development and Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcdd12080282\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080282","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Thirty-Day and One-Year All-Cause Mortality of ST-Segment Elevation Myocardial Infarction in Johannesburg, South Africa: Insights from the STEMI HOC-1 Prospective Study.
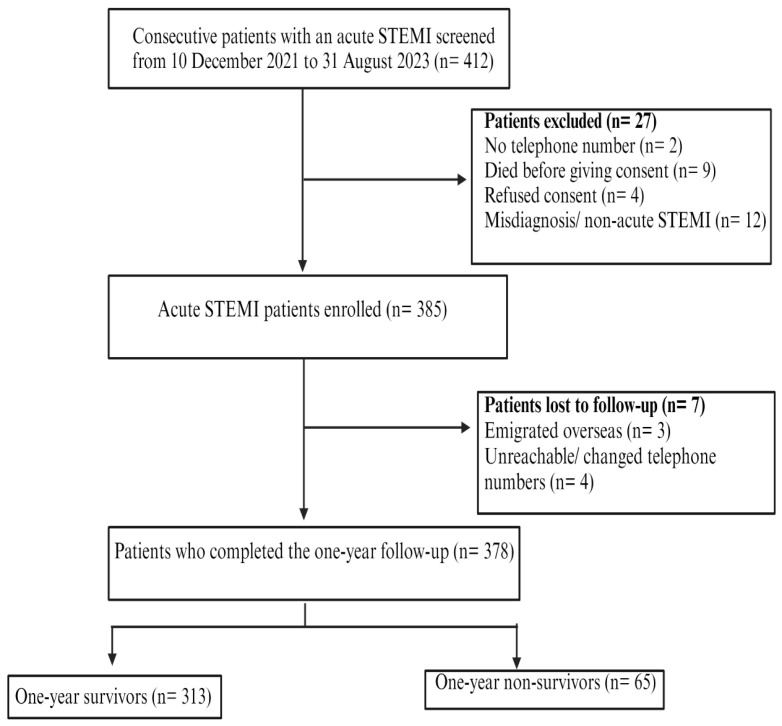
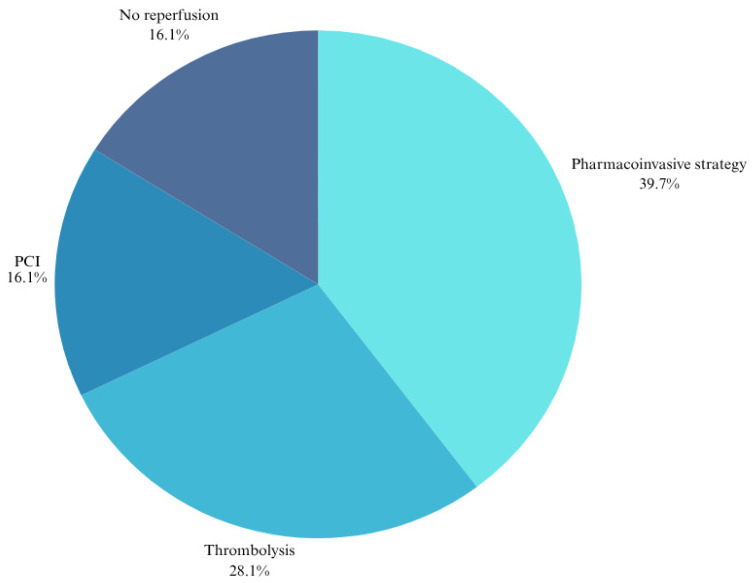
Despite the increased mortality due to ST-segment elevation myocardial infarction (STEMI) in South Africa (SA), SA lacks comprehensive data on STEMI clinical outcomes. This study aimed to determine the 30-day and one-year all-cause mortality rates of STEMI patients presenting to our hospital. This was a one-year prospective single-centre study of STEMI patients presenting to the Charlotte Maxeke Johannesburg Hospital in SA between December 2021 and August 2023. We compared the baseline clinical characteristics, reperfusion strategies, and in-hospital, 30-day, and one-year clinical outcomes of survivors and non-survivors. This cohort included 378 STEMI participants. The in-hospital, 30-day, and one-year all-cause mortality rates were 6.6% (n = 25), 10.1% (n = 38), and 17.2% (n = 65), respectively. The pharmacoinvasive strategy was the most used reperfusion therapy (n = 150, 39.7%). On adjusted multivariate Cox regression analysis, a Killip class >2 was the strongest independent predictor of 30-day [HR 5.61, 95% CI 2.83-11.12; p < 0.001] and one-year all-cause mortality [HR 1.72, 95% CI 1.26-2.34; p = 0.001]. Although mortality has increased, our mortality rates were comparable to outcomes from high-income countries but significantly lower than reports from other low- or middle-income countries. Importantly, there were no significant differences in 30-day and one-year survival outcomes between the different reperfusion strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


