Joseph Kletzer, Maximilian Kreibich, Martin Czerny, Tim Berger, Albi Fagu, Laurin Micek, Ulrich Franke, Matthias Eschenhagen, Tau S Hartikainen, Mirjam Wild, Dalibor Bockelmann
{"title":"以患者血容量为指标的输血对冠状动脉搭桥术后5年死亡率的影响——一项EuroSCORE II调整样条回归分析","authors":"Joseph Kletzer, Maximilian Kreibich, Martin Czerny, Tim Berger, Albi Fagu, Laurin Micek, Ulrich Franke, Matthias Eschenhagen, Tau S Hartikainen, Mirjam Wild, Dalibor Bockelmann","doi":"10.3390/jcdd12080287","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> While timely blood transfusion is critical for restoring oxygen-carrying capacity after coronary artery bypass grafting (CABG), allogeneic blood product transfusions are independently associated with increased long-term mortality, necessitating a risk-stratified approach to balance oxygen delivery against immunological complications and infection risks. <b>Methods:</b> We retrospectively analyzed 3376 patients undergoing isolated CABG between 2005 and 2023 at a single tertiary center. Patients who died during their perioperative hospital stay within 30 days were excluded. Transfusion burden was assessed both as the absolute number of blood product units (packed red blood cells, platelet transfusion, fresh frozen plasma) and as a percentage of calculated patient blood volume. The primary outcome was all-cause mortality at 5 years. Flexible Cox regression with penalized smoothing splines, adjusted for EuroSCORE II, was used to model dose-response relationships. <b>Results:</b> From our cohort of 3376 patients, a total of 137 patients (4.05%) received >10 units of packed red blood cells (PRBC) perioperatively. These patients were older (median 71 vs. 68 years, <i>p</i> < 0.001), more often female (29% vs. 15%, <i>p</i> < 0.001), and had higher preoperative risk (EuroSCORE II: 2.53 vs. 1.41, <i>p</i> < 0.001). After 5 years, mortality was 42% in the massive transfusion group versus 10% in controls. Spline regression revealed an exponential increase in mortality with transfused units: 14 units yielded a 1.5-fold higher hazard of death (HR 1.46, 95% CI 1.31-1.64), rising to HR 2.71 (95% CI 2.12-3.47) at 30 units. When transfusion was indexed to blood volume, this relationship became linear and more tightly correlated with mortality, with lower maximum hazard ratios and narrower confidence intervals. <b>Conclusions:</b> Indexing transfusion burden to the percentage of patient blood volume replaced provides a more accurate and clinically actionable predictor of 5-year mortality after CABG than absolute unit counts. Our findings support a shift toward individualized, volume-based transfusion strategies to optimize patient outcomes and resource stewardship in a time of limited availability of blood products.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387114/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Influence of Blood Transfusion Indexed to Patient Blood Volume on 5-Year Mortality After Coronary Artery Bypass Grafting-An EuroSCORE II Adjusted Spline Regression Analysis.\",\"authors\":\"Joseph Kletzer, Maximilian Kreibich, Martin Czerny, Tim Berger, Albi Fagu, Laurin Micek, Ulrich Franke, Matthias Eschenhagen, Tau S Hartikainen, Mirjam Wild, Dalibor Bockelmann\",\"doi\":\"10.3390/jcdd12080287\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> While timely blood transfusion is critical for restoring oxygen-carrying capacity after coronary artery bypass grafting (CABG), allogeneic blood product transfusions are independently associated with increased long-term mortality, necessitating a risk-stratified approach to balance oxygen delivery against immunological complications and infection risks. <b>Methods:</b> We retrospectively analyzed 3376 patients undergoing isolated CABG between 2005 and 2023 at a single tertiary center. Patients who died during their perioperative hospital stay within 30 days were excluded. Transfusion burden was assessed both as the absolute number of blood product units (packed red blood cells, platelet transfusion, fresh frozen plasma) and as a percentage of calculated patient blood volume. The primary outcome was all-cause mortality at 5 years. Flexible Cox regression with penalized smoothing splines, adjusted for EuroSCORE II, was used to model dose-response relationships. <b>Results:</b> From our cohort of 3376 patients, a total of 137 patients (4.05%) received >10 units of packed red blood cells (PRBC) perioperatively. These patients were older (median 71 vs. 68 years, <i>p</i> < 0.001), more often female (29% vs. 15%, <i>p</i> < 0.001), and had higher preoperative risk (EuroSCORE II: 2.53 vs. 1.41, <i>p</i> < 0.001). After 5 years, mortality was 42% in the massive transfusion group versus 10% in controls. Spline regression revealed an exponential increase in mortality with transfused units: 14 units yielded a 1.5-fold higher hazard of death (HR 1.46, 95% CI 1.31-1.64), rising to HR 2.71 (95% CI 2.12-3.47) at 30 units. When transfusion was indexed to blood volume, this relationship became linear and more tightly correlated with mortality, with lower maximum hazard ratios and narrower confidence intervals. <b>Conclusions:</b> Indexing transfusion burden to the percentage of patient blood volume replaced provides a more accurate and clinically actionable predictor of 5-year mortality after CABG than absolute unit counts. Our findings support a shift toward individualized, volume-based transfusion strategies to optimize patient outcomes and resource stewardship in a time of limited availability of blood products.</p>\",\"PeriodicalId\":15197,\"journal\":{\"name\":\"Journal of Cardiovascular Development and Disease\",\"volume\":\"12 8\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387114/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Development and Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcdd12080287\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080287","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:虽然及时输血对于冠状动脉旁路移植术(CABG)后氧承载能力的恢复至关重要,但异体血液制品输血与长期死亡率的增加独立相关,因此需要采取风险分层的方法来平衡氧输送与免疫并发症和感染风险。方法:我们回顾性分析了2005年至2023年在单一三级中心接受孤立CABG的3376例患者。排除围手术期住院30天内死亡的患者。输血负担以血液制品单位(红细胞、血小板、新鲜冷冻血浆)的绝对数量和占计算患者血量的百分比进行评估。主要结局为5年全因死亡率。采用带有惩罚平滑样条的灵活Cox回归,根据EuroSCORE II进行调整,来模拟剂量-反应关系。结果:在我们的3376例患者队列中,共有137例(4.05%)患者围手术期接受了10个单位的填充红细胞(PRBC)。这些患者年龄较大(中位年龄为71岁对68岁,p < 0.001),多为女性(29%对15%,p < 0.001),术前风险较高(EuroSCORE II: 2.53对1.41,p < 0.001)。5年后,大量输血组的死亡率为42%,对照组为10%。样条回归显示输血单位的死亡率呈指数增长:14单位的死亡风险增加1.5倍(危险比1.46,95% CI 1.31-1.64), 30单位的死亡风险增加到2.71 (95% CI 2.12-3.47)。当输血与血容量挂钩时,这种关系变为线性关系,与死亡率的相关性更强,最大风险比更低,置信区间更窄。结论:与绝对单位计数相比,将输血负担与患者替换血容量的百分比相关联,可以更准确地预测冠状动脉搭桥后5年死亡率。我们的研究结果支持在血液制品供应有限的情况下,向个性化、基于量的输血策略转变,以优化患者预后和资源管理。
The Influence of Blood Transfusion Indexed to Patient Blood Volume on 5-Year Mortality After Coronary Artery Bypass Grafting-An EuroSCORE II Adjusted Spline Regression Analysis.
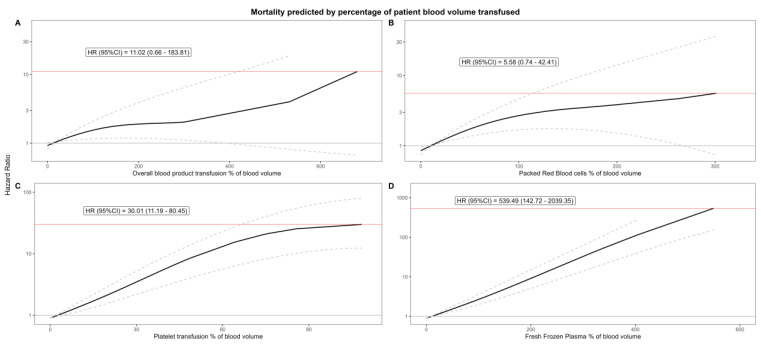
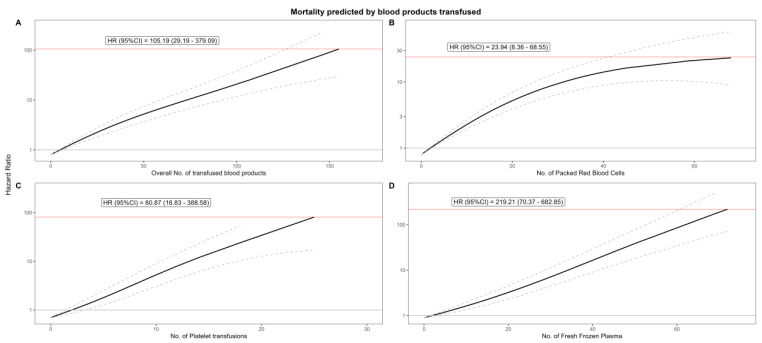
Background: While timely blood transfusion is critical for restoring oxygen-carrying capacity after coronary artery bypass grafting (CABG), allogeneic blood product transfusions are independently associated with increased long-term mortality, necessitating a risk-stratified approach to balance oxygen delivery against immunological complications and infection risks. Methods: We retrospectively analyzed 3376 patients undergoing isolated CABG between 2005 and 2023 at a single tertiary center. Patients who died during their perioperative hospital stay within 30 days were excluded. Transfusion burden was assessed both as the absolute number of blood product units (packed red blood cells, platelet transfusion, fresh frozen plasma) and as a percentage of calculated patient blood volume. The primary outcome was all-cause mortality at 5 years. Flexible Cox regression with penalized smoothing splines, adjusted for EuroSCORE II, was used to model dose-response relationships. Results: From our cohort of 3376 patients, a total of 137 patients (4.05%) received >10 units of packed red blood cells (PRBC) perioperatively. These patients were older (median 71 vs. 68 years, p < 0.001), more often female (29% vs. 15%, p < 0.001), and had higher preoperative risk (EuroSCORE II: 2.53 vs. 1.41, p < 0.001). After 5 years, mortality was 42% in the massive transfusion group versus 10% in controls. Spline regression revealed an exponential increase in mortality with transfused units: 14 units yielded a 1.5-fold higher hazard of death (HR 1.46, 95% CI 1.31-1.64), rising to HR 2.71 (95% CI 2.12-3.47) at 30 units. When transfusion was indexed to blood volume, this relationship became linear and more tightly correlated with mortality, with lower maximum hazard ratios and narrower confidence intervals. Conclusions: Indexing transfusion burden to the percentage of patient blood volume replaced provides a more accurate and clinically actionable predictor of 5-year mortality after CABG than absolute unit counts. Our findings support a shift toward individualized, volume-based transfusion strategies to optimize patient outcomes and resource stewardship in a time of limited availability of blood products.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


