{"title":"复发性心房颤动的电生理底物和肺静脉重连模式:再消融患者热策略的比较。","authors":"Krisztian Istvan Kassa, Adwity Shakya, Zoltan Som, Csaba Foldesi, Attila Kardos","doi":"10.3390/jcdd12080298","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The influence of the initial ablation modality on pulmonary vein (PV) reconnection and substrate characteristics in redo procedures for recurrent atrial fibrillation (AF) remains unclear. We assessed how different thermal strategies-ablation index (AI)-guided radiofrequency (RF) versus cryoballoon (CB) ablation-affect remapping findings during redo pulmonary vein isolation (PVI).</p><p><strong>Methods: </strong>We included patients undergoing redo ablation between 2015 and 2024 with high-density electroanatomic mapping. Initial PVI modalities were retrospectively classified as low-power, long-duration (LPLD) RF; high-power, short-duration (HPSD) RF; or second-/third-generation CB. Reconnection sites were mapped using multielectrode catheters. Redo PVI was performed using AI-guided RF. Segments showing PV reconnection were reisolated; if all PVs remained isolated and AF persisted, posterior wall isolation was performed.</p><p><strong>Results: </strong>Among 195 patients (LPLD: 63; HPSD: 30; CB: 102), complete PVI at redo was observed in 0% (LPLD), 23.3% (HPSD), and 10.1% (CB) (<i>p</i> < 0.01 for LPLD vs. HPSD). Reconnection patterns varied by technique; LPLD primarily affected the right carina, while HPSD and CB showed reconnections at the LSPV ridge. Organized atrial tachycardia was least frequent after CB (12.7%, <i>p</i> < 0.002).</p><p><strong>Conclusion: </strong>Initial ablation strategy significantly influences PV reconnection and post-PVI arrhythmia patterns, with implications for redo procedure planning.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386683/pdf/","citationCount":"0","resultStr":"{\"title\":\"Electrophysiological Substrate and Pulmonary Vein Reconnection Patterns in Recurrent Atrial Fibrillation: Comparing Thermal Strategies in Patients Undergoing Redo Ablation.\",\"authors\":\"Krisztian Istvan Kassa, Adwity Shakya, Zoltan Som, Csaba Foldesi, Attila Kardos\",\"doi\":\"10.3390/jcdd12080298\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The influence of the initial ablation modality on pulmonary vein (PV) reconnection and substrate characteristics in redo procedures for recurrent atrial fibrillation (AF) remains unclear. We assessed how different thermal strategies-ablation index (AI)-guided radiofrequency (RF) versus cryoballoon (CB) ablation-affect remapping findings during redo pulmonary vein isolation (PVI).</p><p><strong>Methods: </strong>We included patients undergoing redo ablation between 2015 and 2024 with high-density electroanatomic mapping. Initial PVI modalities were retrospectively classified as low-power, long-duration (LPLD) RF; high-power, short-duration (HPSD) RF; or second-/third-generation CB. Reconnection sites were mapped using multielectrode catheters. Redo PVI was performed using AI-guided RF. Segments showing PV reconnection were reisolated; if all PVs remained isolated and AF persisted, posterior wall isolation was performed.</p><p><strong>Results: </strong>Among 195 patients (LPLD: 63; HPSD: 30; CB: 102), complete PVI at redo was observed in 0% (LPLD), 23.3% (HPSD), and 10.1% (CB) (<i>p</i> < 0.01 for LPLD vs. HPSD). Reconnection patterns varied by technique; LPLD primarily affected the right carina, while HPSD and CB showed reconnections at the LSPV ridge. Organized atrial tachycardia was least frequent after CB (12.7%, <i>p</i> < 0.002).</p><p><strong>Conclusion: </strong>Initial ablation strategy significantly influences PV reconnection and post-PVI arrhythmia patterns, with implications for redo procedure planning.</p>\",\"PeriodicalId\":15197,\"journal\":{\"name\":\"Journal of Cardiovascular Development and Disease\",\"volume\":\"12 8\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386683/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Development and Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcdd12080298\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080298","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:在复发性心房颤动(AF)的重做手术中,初始消融方式对肺静脉(PV)重连和底物特征的影响尚不清楚。我们评估了不同的热策略-消融指数(AI)引导射频(RF)与低温球囊(CB)消融-如何影响重做肺静脉隔离(PVI)期间的重新定位结果。方法:我们纳入了2015年至2024年间接受高密度电解剖测绘的重做消融的患者。最初的PVI模式被回顾性分类为低功率,长时间(LPLD) RF;高功率、短持续时间(HPSD)射频;或第二/第三代CB。使用多电极导管绘制重连位点。使用人工智能引导射频重新进行PVI。重新隔离显示PV重连的节段;如果所有pv保持孤立且AF持续存在,则进行后壁隔离。结果:195例患者(LPLD: 63例;HPSD: 30例;CB: 102例)中,重做时完全PVI的比例分别为0% (LPLD)、23.3% (HPSD)和10.1% (CB) (LPLD vs HPSD p < 0.01)。重连模式因技术而异;LPLD主要影响右隆突,而HPSD和CB在LSPV脊处显示重连。术后有组织性房性心动过速发生率最低(12.7%,p < 0.002)。结论:初始消融策略显著影响PV再连接和pvi后心律失常模式,对重做手术计划具有指导意义。
Electrophysiological Substrate and Pulmonary Vein Reconnection Patterns in Recurrent Atrial Fibrillation: Comparing Thermal Strategies in Patients Undergoing Redo Ablation.
Background: The influence of the initial ablation modality on pulmonary vein (PV) reconnection and substrate characteristics in redo procedures for recurrent atrial fibrillation (AF) remains unclear. We assessed how different thermal strategies-ablation index (AI)-guided radiofrequency (RF) versus cryoballoon (CB) ablation-affect remapping findings during redo pulmonary vein isolation (PVI).
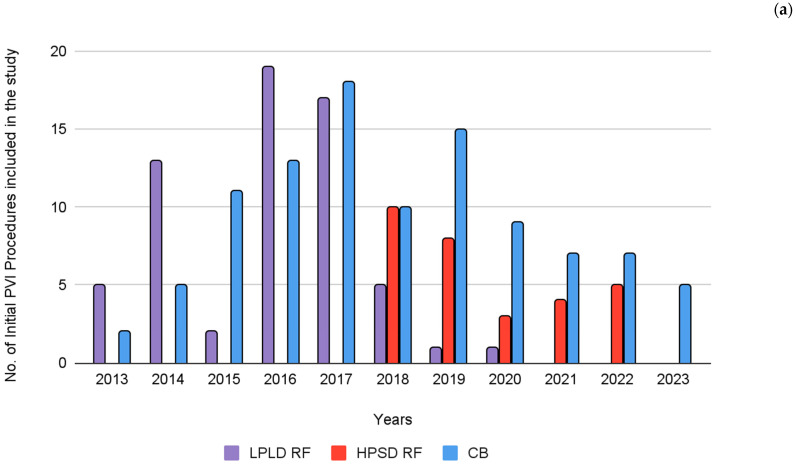
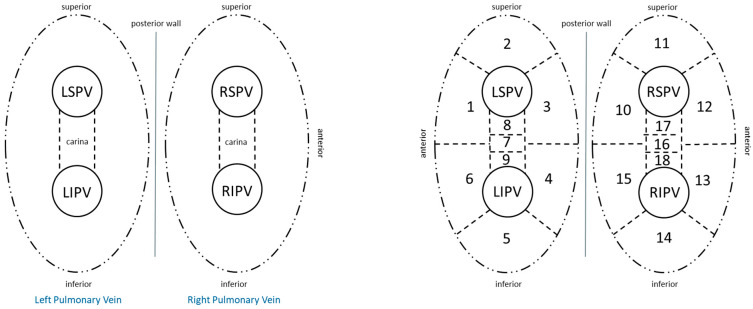
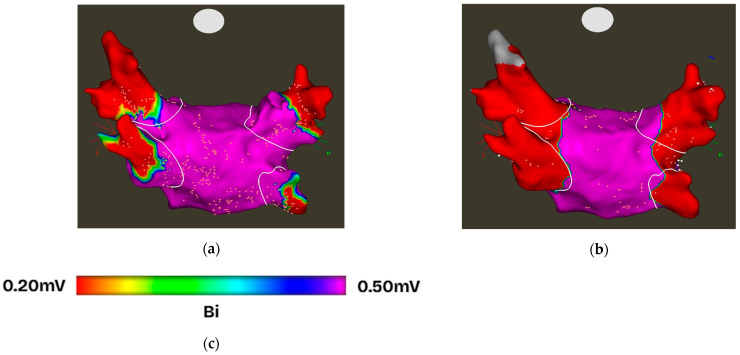
Methods: We included patients undergoing redo ablation between 2015 and 2024 with high-density electroanatomic mapping. Initial PVI modalities were retrospectively classified as low-power, long-duration (LPLD) RF; high-power, short-duration (HPSD) RF; or second-/third-generation CB. Reconnection sites were mapped using multielectrode catheters. Redo PVI was performed using AI-guided RF. Segments showing PV reconnection were reisolated; if all PVs remained isolated and AF persisted, posterior wall isolation was performed.
Results: Among 195 patients (LPLD: 63; HPSD: 30; CB: 102), complete PVI at redo was observed in 0% (LPLD), 23.3% (HPSD), and 10.1% (CB) (p < 0.01 for LPLD vs. HPSD). Reconnection patterns varied by technique; LPLD primarily affected the right carina, while HPSD and CB showed reconnections at the LSPV ridge. Organized atrial tachycardia was least frequent after CB (12.7%, p < 0.002).
Conclusion: Initial ablation strategy significantly influences PV reconnection and post-PVI arrhythmia patterns, with implications for redo procedure planning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


