Robert L Ferris, Rom S Leidner, Christine H Chung, Antonio Jimeno, Sylvia M Lee, Ammar Sukari, Jorge J Nieva, Juneko E Grilley-Olson, Rebecca Redman, Stuart J Wong, Victoria M Villaflor, Jamal Misleh, Friedrich Graf Finckenstein, Jeffrey Chou, Brian Gastman, Rana Fiaz, Melissa Catlett, Min Yi, Ezra E W Cohen
{"title":"一次性自体肿瘤浸润性淋巴细胞治疗复发性和/或转移性头颈部鳞状细胞癌的疗效和安全性。","authors":"Robert L Ferris, Rom S Leidner, Christine H Chung, Antonio Jimeno, Sylvia M Lee, Ammar Sukari, Jorge J Nieva, Juneko E Grilley-Olson, Rebecca Redman, Stuart J Wong, Victoria M Villaflor, Jamal Misleh, Friedrich Graf Finckenstein, Jeffrey Chou, Brian Gastman, Rana Fiaz, Melissa Catlett, Min Yi, Ezra E W Cohen","doi":"10.1136/jitc-2025-011633","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recurrent and/or metastatic head and neck squamous cell carcinoma (HNSCC) has a high recurrence rate after first-line immunotherapy or chemoimmunotherapy. The presence of a high density of tumor-infiltrating lymphocytes (TILs) in HNSCC tumors was shown to be associated with improved clinical outcomes. One-time autologous TIL cell therapy was evaluated in patients with recurrent and/or metastatic HNSCC.</p><p><strong>Methods: </strong>C-145-03 (NCT03083873) was a phase 2 study of TIL in patients with recurrent and/or metastatic HNSCC assigned to 1 of 4 treatment cohorts: cohort 1, non-cryopreserved TIL; cohort 2, cryopreserved lifileucel (22-day manufacturing); cohort 3, cryopreserved lifileucel (16-day manufacturing); cohort 4, cryopreserved LN-145-S1 programmed cell death protein-1 (PD-1) selected. Patients underwent tumor resection for TIL generation. After preparative non-myeloablative lymphodepletion, patients received a single infusion of TIL followed by interleukin-2 (IL-2) infusion(s). The primary endpoint was investigator-assessed objective response rate (ORR) per Response Evaluation Criteria for Solid Tumors (RECIST) V.1.1. Secondary endpoints were investigator-assessed duration of response (DOR), disease control rate (DCR), progression-free survival, overall survival, and incidence of treatment-emergent adverse events.</p><p><strong>Results: </strong>Overall, 53 patients received TIL: cohort 1 (n=8), cohort 2 (n=17), cohort 3 (n=16), cohort 4 (n=12). Median age was 57 years and most patients were males (87%; 46/53) with stage IV disease (98%; 52/53). Patients had a median of two prior lines of systemic therapy; 87% (46/53) of patients had prior anti-PD-1/programmed cell death ligand-1 therapy and 72% (38/53) had prior chemotherapy. The ORR was 11% (6/53) with six patients achieving partial response (cohort 1, n=3; cohort 2, n=1; cohort 4, n=2). At median follow-up of 17.9 months, the median DOR was 7.6 months. The DCR was 76% (40/53); 64% (34/53) of patients had stable disease. The safety profile was consistent with known toxicities associated with non-myeloablative lymphodepletion and IL-2 administration.</p><p><strong>Conclusions: </strong>This study demonstrated the feasibility of consistently generating sufficient TIL from HNSCC tumors. Results from this study suggest TIL cell therapy may serve as a potential treatment option for patients with HNSCC and support further development, including TIL cell therapy combined with immune checkpoint inhibitors or other agents or with other TIL products.</p><p><strong>Trial registration number: </strong>NCT03083873.</p>","PeriodicalId":14820,"journal":{"name":"Journal for Immunotherapy of Cancer","volume":"13 8","pages":""},"PeriodicalIF":10.6000,"publicationDate":"2025-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382571/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and safety of one-time autologous tumor-infiltrating lymphocyte cell therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma.\",\"authors\":\"Robert L Ferris, Rom S Leidner, Christine H Chung, Antonio Jimeno, Sylvia M Lee, Ammar Sukari, Jorge J Nieva, Juneko E Grilley-Olson, Rebecca Redman, Stuart J Wong, Victoria M Villaflor, Jamal Misleh, Friedrich Graf Finckenstein, Jeffrey Chou, Brian Gastman, Rana Fiaz, Melissa Catlett, Min Yi, Ezra E W Cohen\",\"doi\":\"10.1136/jitc-2025-011633\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Recurrent and/or metastatic head and neck squamous cell carcinoma (HNSCC) has a high recurrence rate after first-line immunotherapy or chemoimmunotherapy. The presence of a high density of tumor-infiltrating lymphocytes (TILs) in HNSCC tumors was shown to be associated with improved clinical outcomes. One-time autologous TIL cell therapy was evaluated in patients with recurrent and/or metastatic HNSCC.</p><p><strong>Methods: </strong>C-145-03 (NCT03083873) was a phase 2 study of TIL in patients with recurrent and/or metastatic HNSCC assigned to 1 of 4 treatment cohorts: cohort 1, non-cryopreserved TIL; cohort 2, cryopreserved lifileucel (22-day manufacturing); cohort 3, cryopreserved lifileucel (16-day manufacturing); cohort 4, cryopreserved LN-145-S1 programmed cell death protein-1 (PD-1) selected. Patients underwent tumor resection for TIL generation. After preparative non-myeloablative lymphodepletion, patients received a single infusion of TIL followed by interleukin-2 (IL-2) infusion(s). The primary endpoint was investigator-assessed objective response rate (ORR) per Response Evaluation Criteria for Solid Tumors (RECIST) V.1.1. Secondary endpoints were investigator-assessed duration of response (DOR), disease control rate (DCR), progression-free survival, overall survival, and incidence of treatment-emergent adverse events.</p><p><strong>Results: </strong>Overall, 53 patients received TIL: cohort 1 (n=8), cohort 2 (n=17), cohort 3 (n=16), cohort 4 (n=12). Median age was 57 years and most patients were males (87%; 46/53) with stage IV disease (98%; 52/53). Patients had a median of two prior lines of systemic therapy; 87% (46/53) of patients had prior anti-PD-1/programmed cell death ligand-1 therapy and 72% (38/53) had prior chemotherapy. The ORR was 11% (6/53) with six patients achieving partial response (cohort 1, n=3; cohort 2, n=1; cohort 4, n=2). At median follow-up of 17.9 months, the median DOR was 7.6 months. The DCR was 76% (40/53); 64% (34/53) of patients had stable disease. The safety profile was consistent with known toxicities associated with non-myeloablative lymphodepletion and IL-2 administration.</p><p><strong>Conclusions: </strong>This study demonstrated the feasibility of consistently generating sufficient TIL from HNSCC tumors. Results from this study suggest TIL cell therapy may serve as a potential treatment option for patients with HNSCC and support further development, including TIL cell therapy combined with immune checkpoint inhibitors or other agents or with other TIL products.</p><p><strong>Trial registration number: </strong>NCT03083873.</p>\",\"PeriodicalId\":14820,\"journal\":{\"name\":\"Journal for Immunotherapy of Cancer\",\"volume\":\"13 8\",\"pages\":\"\"},\"PeriodicalIF\":10.6000,\"publicationDate\":\"2025-08-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382571/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal for Immunotherapy of Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/jitc-2025-011633\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal for Immunotherapy of Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/jitc-2025-011633","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Efficacy and safety of one-time autologous tumor-infiltrating lymphocyte cell therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma.
Background: Recurrent and/or metastatic head and neck squamous cell carcinoma (HNSCC) has a high recurrence rate after first-line immunotherapy or chemoimmunotherapy. The presence of a high density of tumor-infiltrating lymphocytes (TILs) in HNSCC tumors was shown to be associated with improved clinical outcomes. One-time autologous TIL cell therapy was evaluated in patients with recurrent and/or metastatic HNSCC.
Methods: C-145-03 (NCT03083873) was a phase 2 study of TIL in patients with recurrent and/or metastatic HNSCC assigned to 1 of 4 treatment cohorts: cohort 1, non-cryopreserved TIL; cohort 2, cryopreserved lifileucel (22-day manufacturing); cohort 3, cryopreserved lifileucel (16-day manufacturing); cohort 4, cryopreserved LN-145-S1 programmed cell death protein-1 (PD-1) selected. Patients underwent tumor resection for TIL generation. After preparative non-myeloablative lymphodepletion, patients received a single infusion of TIL followed by interleukin-2 (IL-2) infusion(s). The primary endpoint was investigator-assessed objective response rate (ORR) per Response Evaluation Criteria for Solid Tumors (RECIST) V.1.1. Secondary endpoints were investigator-assessed duration of response (DOR), disease control rate (DCR), progression-free survival, overall survival, and incidence of treatment-emergent adverse events.
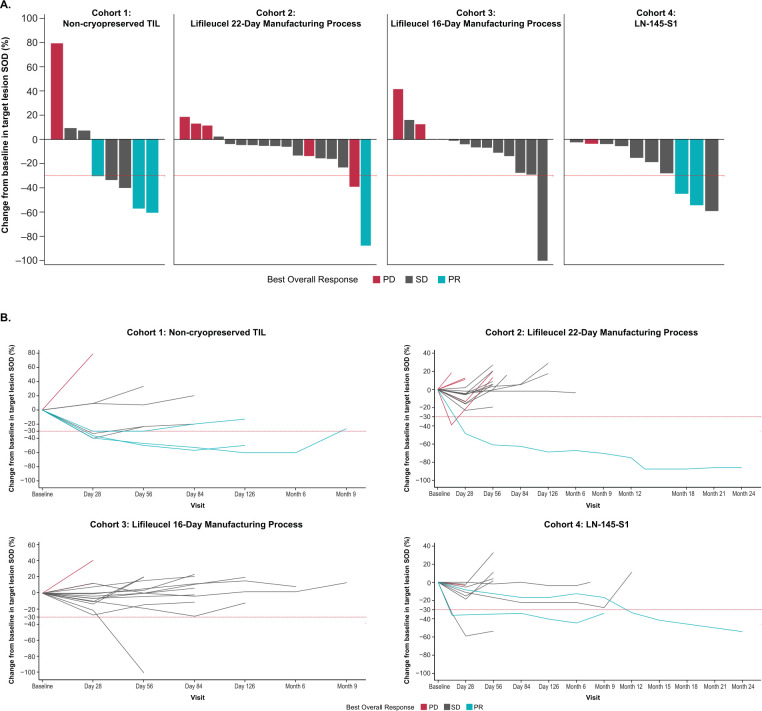
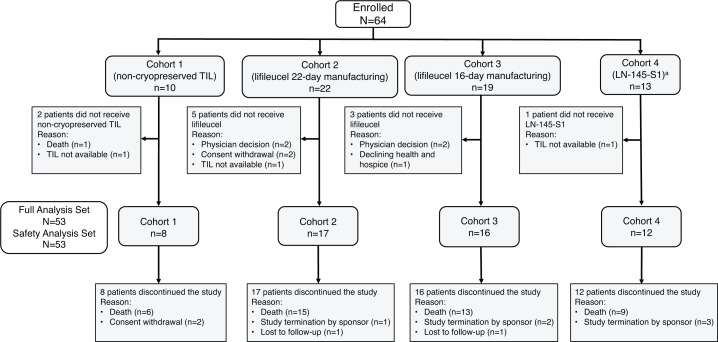
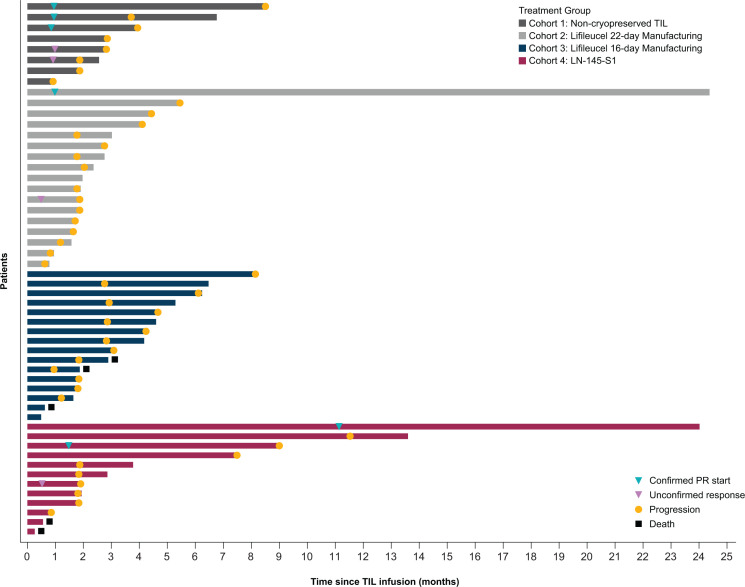
Results: Overall, 53 patients received TIL: cohort 1 (n=8), cohort 2 (n=17), cohort 3 (n=16), cohort 4 (n=12). Median age was 57 years and most patients were males (87%; 46/53) with stage IV disease (98%; 52/53). Patients had a median of two prior lines of systemic therapy; 87% (46/53) of patients had prior anti-PD-1/programmed cell death ligand-1 therapy and 72% (38/53) had prior chemotherapy. The ORR was 11% (6/53) with six patients achieving partial response (cohort 1, n=3; cohort 2, n=1; cohort 4, n=2). At median follow-up of 17.9 months, the median DOR was 7.6 months. The DCR was 76% (40/53); 64% (34/53) of patients had stable disease. The safety profile was consistent with known toxicities associated with non-myeloablative lymphodepletion and IL-2 administration.
Conclusions: This study demonstrated the feasibility of consistently generating sufficient TIL from HNSCC tumors. Results from this study suggest TIL cell therapy may serve as a potential treatment option for patients with HNSCC and support further development, including TIL cell therapy combined with immune checkpoint inhibitors or other agents or with other TIL products.
期刊介绍:
The Journal for ImmunoTherapy of Cancer (JITC) is a peer-reviewed publication that promotes scientific exchange and deepens knowledge in the constantly evolving fields of tumor immunology and cancer immunotherapy. With an open access format, JITC encourages widespread access to its findings. The journal covers a wide range of topics, spanning from basic science to translational and clinical research. Key areas of interest include tumor-host interactions, the intricate tumor microenvironment, animal models, the identification of predictive and prognostic immune biomarkers, groundbreaking pharmaceutical and cellular therapies, innovative vaccines, combination immune-based treatments, and the study of immune-related toxicity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


