Adalgisa Fastuca, Antonio Vergori, Giuseppe Robustelli, Chiara Piccolo, Maria Ragazzo, Maddalena Marinoni, Massimo Agosti
{"title":"葡萄糖-6-磷酸脱氢酶缺乏引起溶血性贫血和高铁血红蛋白血症:1例7岁女性患者报告。","authors":"Adalgisa Fastuca, Antonio Vergori, Giuseppe Robustelli, Chiara Piccolo, Maria Ragazzo, Maddalena Marinoni, Massimo Agosti","doi":"10.1186/s13052-025-02051-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients affected by glucose-6-phosphate dehydrogenase (G6PDH) deficiency are often asymptomatic until an oxidative stress occurs, causing acute hemolytic anemia. The coexistence of hemolytic crisis secondary to G6PDH deficiency and methemoglobinemia is an already known phenomenon, especially after the ingestion of fava beans. While past literature described this association primarily in adult patients, it remains an unusual finding in pediatric population. Our patient's age, as long as her gender, and a negative family history represent, indeed, the peculiarity of what we described.</p><p><strong>Case presentation: </strong>We present the case of a 7-year-old female patient with a clinical history of hyperpyrexia, several episodes of yellowish vomit, hypercromic urine, loose stools, asthenia with jaundice. At home paracetamol and a single dose of ibuprofen were administered. No recent history of fava bean ingestion or relevant events were reported in physiological and pathological anamnesis. Family history was negative for hematological comorbidities. Blood tests performed at the emergency room showed a picture of severe anemia with negative direct and indirect Coombs tests, mild acute renal failure, increased inflammation markers and a methemoglobin level equal to 13.7% on blood gas analysis. The detection of vital parameters showed O2-Sat equal to 75% without signs of respiratory distress. A broad-spectrum antibiotic therapy with ceftriaxone and oxygen-therapy were administered, hospitalization was then arranged. Immune-mediated anemia and lymphoproliferative diseases were excluded. G6PDH dosage was requested, resulting indicative of deficiency. Fecal virus testing revealed a positivity for Norovirus. Transfusions of red cell concentrates (RCC) were performed, and the methemoglobin value gradually decreased with stabilization of the hemoglobin, so that methylene blue therapy was not administrated. The patient's clinical conditions improved in almost 5 days.</p><p><strong>Conclusions: </strong>When G6PDH deficiency and methemoglobinemia coexist, a prompt diagnosis is essential. The administration of methylene blue, therapy of choice for the treatment of methemoglobinemia, in fact, may cause a worsening of hemolytic crises in patients affected by G6PDH deficiency. Considering our patient's clinical features, not clearly evocative of G6PDH deficiency, this case represented a challenge for both diagnosis and treatment, reminding to always consider G6PDH deficiency in case of hemolytic anemia associated with methemoglobinemia.</p>","PeriodicalId":14511,"journal":{"name":"Italian Journal of Pediatrics","volume":"51 1","pages":"258"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12369025/pdf/","citationCount":"0","resultStr":"{\"title\":\"Glucose-6-phosphate dehydrogenase deficiency induced hemolytic anemia and methemoglobinemia: a case report in a 7 -year-old female patient.\",\"authors\":\"Adalgisa Fastuca, Antonio Vergori, Giuseppe Robustelli, Chiara Piccolo, Maria Ragazzo, Maddalena Marinoni, Massimo Agosti\",\"doi\":\"10.1186/s13052-025-02051-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients affected by glucose-6-phosphate dehydrogenase (G6PDH) deficiency are often asymptomatic until an oxidative stress occurs, causing acute hemolytic anemia. The coexistence of hemolytic crisis secondary to G6PDH deficiency and methemoglobinemia is an already known phenomenon, especially after the ingestion of fava beans. While past literature described this association primarily in adult patients, it remains an unusual finding in pediatric population. Our patient's age, as long as her gender, and a negative family history represent, indeed, the peculiarity of what we described.</p><p><strong>Case presentation: </strong>We present the case of a 7-year-old female patient with a clinical history of hyperpyrexia, several episodes of yellowish vomit, hypercromic urine, loose stools, asthenia with jaundice. At home paracetamol and a single dose of ibuprofen were administered. No recent history of fava bean ingestion or relevant events were reported in physiological and pathological anamnesis. Family history was negative for hematological comorbidities. Blood tests performed at the emergency room showed a picture of severe anemia with negative direct and indirect Coombs tests, mild acute renal failure, increased inflammation markers and a methemoglobin level equal to 13.7% on blood gas analysis. The detection of vital parameters showed O2-Sat equal to 75% without signs of respiratory distress. A broad-spectrum antibiotic therapy with ceftriaxone and oxygen-therapy were administered, hospitalization was then arranged. Immune-mediated anemia and lymphoproliferative diseases were excluded. G6PDH dosage was requested, resulting indicative of deficiency. Fecal virus testing revealed a positivity for Norovirus. Transfusions of red cell concentrates (RCC) were performed, and the methemoglobin value gradually decreased with stabilization of the hemoglobin, so that methylene blue therapy was not administrated. The patient's clinical conditions improved in almost 5 days.</p><p><strong>Conclusions: </strong>When G6PDH deficiency and methemoglobinemia coexist, a prompt diagnosis is essential. The administration of methylene blue, therapy of choice for the treatment of methemoglobinemia, in fact, may cause a worsening of hemolytic crises in patients affected by G6PDH deficiency. Considering our patient's clinical features, not clearly evocative of G6PDH deficiency, this case represented a challenge for both diagnosis and treatment, reminding to always consider G6PDH deficiency in case of hemolytic anemia associated with methemoglobinemia.</p>\",\"PeriodicalId\":14511,\"journal\":{\"name\":\"Italian Journal of Pediatrics\",\"volume\":\"51 1\",\"pages\":\"258\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12369025/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Italian Journal of Pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13052-025-02051-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Italian Journal of Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13052-025-02051-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
Glucose-6-phosphate dehydrogenase deficiency induced hemolytic anemia and methemoglobinemia: a case report in a 7 -year-old female patient.
Background: Patients affected by glucose-6-phosphate dehydrogenase (G6PDH) deficiency are often asymptomatic until an oxidative stress occurs, causing acute hemolytic anemia. The coexistence of hemolytic crisis secondary to G6PDH deficiency and methemoglobinemia is an already known phenomenon, especially after the ingestion of fava beans. While past literature described this association primarily in adult patients, it remains an unusual finding in pediatric population. Our patient's age, as long as her gender, and a negative family history represent, indeed, the peculiarity of what we described.
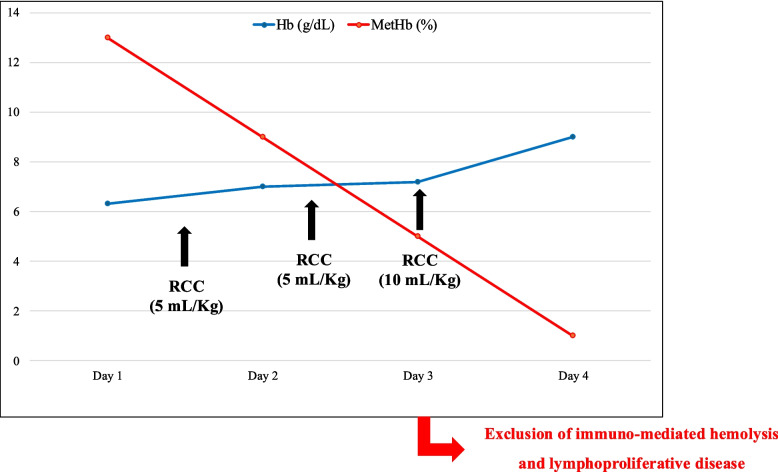
Case presentation: We present the case of a 7-year-old female patient with a clinical history of hyperpyrexia, several episodes of yellowish vomit, hypercromic urine, loose stools, asthenia with jaundice. At home paracetamol and a single dose of ibuprofen were administered. No recent history of fava bean ingestion or relevant events were reported in physiological and pathological anamnesis. Family history was negative for hematological comorbidities. Blood tests performed at the emergency room showed a picture of severe anemia with negative direct and indirect Coombs tests, mild acute renal failure, increased inflammation markers and a methemoglobin level equal to 13.7% on blood gas analysis. The detection of vital parameters showed O2-Sat equal to 75% without signs of respiratory distress. A broad-spectrum antibiotic therapy with ceftriaxone and oxygen-therapy were administered, hospitalization was then arranged. Immune-mediated anemia and lymphoproliferative diseases were excluded. G6PDH dosage was requested, resulting indicative of deficiency. Fecal virus testing revealed a positivity for Norovirus. Transfusions of red cell concentrates (RCC) were performed, and the methemoglobin value gradually decreased with stabilization of the hemoglobin, so that methylene blue therapy was not administrated. The patient's clinical conditions improved in almost 5 days.
Conclusions: When G6PDH deficiency and methemoglobinemia coexist, a prompt diagnosis is essential. The administration of methylene blue, therapy of choice for the treatment of methemoglobinemia, in fact, may cause a worsening of hemolytic crises in patients affected by G6PDH deficiency. Considering our patient's clinical features, not clearly evocative of G6PDH deficiency, this case represented a challenge for both diagnosis and treatment, reminding to always consider G6PDH deficiency in case of hemolytic anemia associated with methemoglobinemia.
期刊介绍:
Italian Journal of Pediatrics is an open access peer-reviewed journal that includes all aspects of pediatric medicine. The journal also covers health service and public health research that addresses primary care issues.
The journal provides a high-quality forum for pediatricians and other healthcare professionals to report and discuss up-to-the-minute research and expert reviews in the field of pediatric medicine. The journal will continue to develop the range of articles published to enable this invaluable resource to stay at the forefront of the field.
Italian Journal of Pediatrics, which commenced in 1975 as Rivista Italiana di Pediatria, provides a high-quality forum for pediatricians and other healthcare professionals to report and discuss up-to-the-minute research and expert reviews in the field of pediatric medicine. The journal will continue to develop the range of articles published to enable this invaluable resource to stay at the forefront of the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


