Lorenzo Calabró, Filippo Annoni, Fabio Silvio Taccone
{"title":"多巴酚丁胺管理:标准化方法的建议。","authors":"Lorenzo Calabró, Filippo Annoni, Fabio Silvio Taccone","doi":"10.1186/s40635-025-00804-1","DOIUrl":null,"url":null,"abstract":"<p><p>Dobutamine is the most commonly used inotropic agent in critically ill patients with impaired cardiac contractility. However, its benefit-risk profile remains debated, and clear, structured guidance for its use is lacking. This hypothesis proposes a pragmatic framework for dobutamine administration to promote rational and consistent clinical and experimental practice. The aim is to propose a rational and reproducible use of inotropic therapy with dobutamine in both clinical and experimental settings in cases of shock with low cardiac output, particularly cardiogenic shock, septic shock with septic cardiomyopathy, and low cardiac output syndrome after cardiac surgery (LCOS). Dobutamine should be prescribed only in the presence of acute circulatory failure with signs of peripheral hypoperfusion and impaired cardiac contractility. A low cardiac index (CI) alone does not mandate inotrope initiation. Echocardiography is essential for initial assessment but should be complemented by continuous cardiac output monitoring for evaluating dose-response. The recommended starting dose is 2.5 μg/kg*min, with stepwise titration based on CI and perfusion markers reassessed every 20 min. A significant CI increase and resolution of hypoperfusion should guide further escalation. Persistent hypoperfusion despite CI improvement may indicate inadequate response and justify cautious dose increases, while continued hypoperfusion with further CI rise suggests a flow-independent deficit, discouraging further titration. Dobutamine should be used with clear indications, guided by a standardized approach integrating continuous hemodynamic and perfusion monitoring. This strategy may help optimize therapeutic benefit while minimizing unnecessary exposure and adverse effects.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"89"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399504/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dobutamine administration: a proposal for a standardized approach.\",\"authors\":\"Lorenzo Calabró, Filippo Annoni, Fabio Silvio Taccone\",\"doi\":\"10.1186/s40635-025-00804-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Dobutamine is the most commonly used inotropic agent in critically ill patients with impaired cardiac contractility. However, its benefit-risk profile remains debated, and clear, structured guidance for its use is lacking. This hypothesis proposes a pragmatic framework for dobutamine administration to promote rational and consistent clinical and experimental practice. The aim is to propose a rational and reproducible use of inotropic therapy with dobutamine in both clinical and experimental settings in cases of shock with low cardiac output, particularly cardiogenic shock, septic shock with septic cardiomyopathy, and low cardiac output syndrome after cardiac surgery (LCOS). Dobutamine should be prescribed only in the presence of acute circulatory failure with signs of peripheral hypoperfusion and impaired cardiac contractility. A low cardiac index (CI) alone does not mandate inotrope initiation. Echocardiography is essential for initial assessment but should be complemented by continuous cardiac output monitoring for evaluating dose-response. The recommended starting dose is 2.5 μg/kg*min, with stepwise titration based on CI and perfusion markers reassessed every 20 min. A significant CI increase and resolution of hypoperfusion should guide further escalation. Persistent hypoperfusion despite CI improvement may indicate inadequate response and justify cautious dose increases, while continued hypoperfusion with further CI rise suggests a flow-independent deficit, discouraging further titration. Dobutamine should be used with clear indications, guided by a standardized approach integrating continuous hemodynamic and perfusion monitoring. This strategy may help optimize therapeutic benefit while minimizing unnecessary exposure and adverse effects.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"89\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399504/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00804-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00804-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Dobutamine administration: a proposal for a standardized approach.
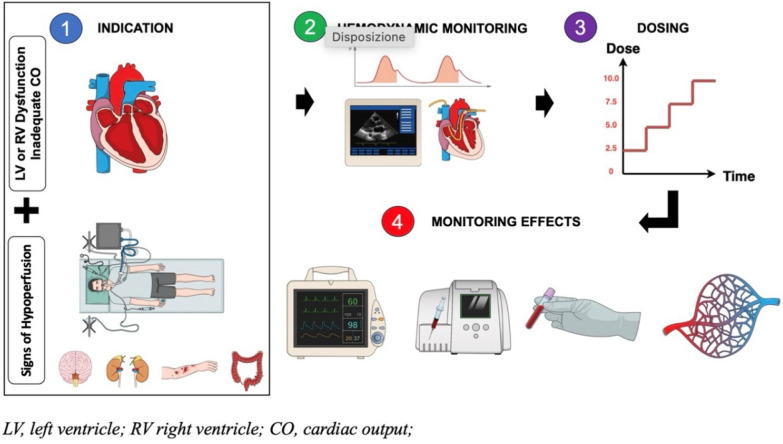
Dobutamine is the most commonly used inotropic agent in critically ill patients with impaired cardiac contractility. However, its benefit-risk profile remains debated, and clear, structured guidance for its use is lacking. This hypothesis proposes a pragmatic framework for dobutamine administration to promote rational and consistent clinical and experimental practice. The aim is to propose a rational and reproducible use of inotropic therapy with dobutamine in both clinical and experimental settings in cases of shock with low cardiac output, particularly cardiogenic shock, septic shock with septic cardiomyopathy, and low cardiac output syndrome after cardiac surgery (LCOS). Dobutamine should be prescribed only in the presence of acute circulatory failure with signs of peripheral hypoperfusion and impaired cardiac contractility. A low cardiac index (CI) alone does not mandate inotrope initiation. Echocardiography is essential for initial assessment but should be complemented by continuous cardiac output monitoring for evaluating dose-response. The recommended starting dose is 2.5 μg/kg*min, with stepwise titration based on CI and perfusion markers reassessed every 20 min. A significant CI increase and resolution of hypoperfusion should guide further escalation. Persistent hypoperfusion despite CI improvement may indicate inadequate response and justify cautious dose increases, while continued hypoperfusion with further CI rise suggests a flow-independent deficit, discouraging further titration. Dobutamine should be used with clear indications, guided by a standardized approach integrating continuous hemodynamic and perfusion monitoring. This strategy may help optimize therapeutic benefit while minimizing unnecessary exposure and adverse effects.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


