Emma Håstad, Riina Aarnio, Lovisa Bergengren, Matts Olovsson
{"title":"HPV检测作为宫颈环切除治疗后治愈的测试:一项基于登记的回顾性队列研究。","authors":"Emma Håstad, Riina Aarnio, Lovisa Bergengren, Matts Olovsson","doi":"10.1186/s13027-025-00690-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Women treated with cervical loop electrosurgical excision procedure require follow-up to detect residual or recurrent HSIL+, defined as high-grade squamous intraepithelial lesions, adenocarcinoma in situ or cervical cancer. Currently, co-testing with cytology and human papillomavirus (HPV) analysis is usually recommended. This study investigates whether HPV testing alone is comparable to co-testing in detecting HSIL + up to three years after treatment. Recurrence rates of HSIL + are also presented, with follow-up extending up to 18 years.</p><p><strong>Methods: </strong>This retrospective cohort study included all 3,540 women treated with a cervical excision in Uppsala County between 1 January 2005 and 31 December 2019. Women with cancer identified in the cone biopsy were excluded. The main outcome was HSIL + detected within three years of follow-up. Sensitivity, specificity and negative predictive value were calculated for the 1,938 women who had a co-testing result as part of their test of cure. Thus, the analysis for the main outcome could finally be performed on 1,938 out of the total number of 3,540 women. Additionally, long-term data on recurrence and time to HSIL+, along with a separate analysis of results prior to cervical cancer diagnosis, were collected for the whole cohort of 3,399 women.</p><p><strong>Results: </strong>The sensitivity and negative predictive value for detecting HSIL + were 69% and 97% for HPV alone, and 74% and 98% for co-testing, respectively. These differences were not statistically significant. Specificity was higher for HPV alone than for co-testing. The negative predictive value of HPV testing for excluding cervical cancer (n = 5) within three years was 100%. Recurrence rate of HSIL + in the three-year follow up was 8%, and the total recurrence rate of HSIL + with a mean follow-up of nine years was 10%. Mean time to recurrence was 28 months. None of 19 cervical cancer cases identified in the long-term follow-up had a co-testing result showing negative HPV but positive cytology.</p><p><strong>Conclusions: </strong>HPV testing alone, as a single test, is comparable to co-testing in detecting HSIL + up to three years after treatment independently of margin status, and demonstrates a higher specificity. Cytology plays a very limited role in the test of cure analysis and could therefore be omitted.</p>","PeriodicalId":13568,"journal":{"name":"Infectious Agents and Cancer","volume":"20 1","pages":"59"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392528/pdf/","citationCount":"0","resultStr":"{\"title\":\"HPV testing alone as a test of cure after treatment with cervical loop excision: a retrospective register-based cohort study.\",\"authors\":\"Emma Håstad, Riina Aarnio, Lovisa Bergengren, Matts Olovsson\",\"doi\":\"10.1186/s13027-025-00690-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Women treated with cervical loop electrosurgical excision procedure require follow-up to detect residual or recurrent HSIL+, defined as high-grade squamous intraepithelial lesions, adenocarcinoma in situ or cervical cancer. Currently, co-testing with cytology and human papillomavirus (HPV) analysis is usually recommended. This study investigates whether HPV testing alone is comparable to co-testing in detecting HSIL + up to three years after treatment. Recurrence rates of HSIL + are also presented, with follow-up extending up to 18 years.</p><p><strong>Methods: </strong>This retrospective cohort study included all 3,540 women treated with a cervical excision in Uppsala County between 1 January 2005 and 31 December 2019. Women with cancer identified in the cone biopsy were excluded. The main outcome was HSIL + detected within three years of follow-up. Sensitivity, specificity and negative predictive value were calculated for the 1,938 women who had a co-testing result as part of their test of cure. Thus, the analysis for the main outcome could finally be performed on 1,938 out of the total number of 3,540 women. Additionally, long-term data on recurrence and time to HSIL+, along with a separate analysis of results prior to cervical cancer diagnosis, were collected for the whole cohort of 3,399 women.</p><p><strong>Results: </strong>The sensitivity and negative predictive value for detecting HSIL + were 69% and 97% for HPV alone, and 74% and 98% for co-testing, respectively. These differences were not statistically significant. Specificity was higher for HPV alone than for co-testing. The negative predictive value of HPV testing for excluding cervical cancer (n = 5) within three years was 100%. Recurrence rate of HSIL + in the three-year follow up was 8%, and the total recurrence rate of HSIL + with a mean follow-up of nine years was 10%. Mean time to recurrence was 28 months. None of 19 cervical cancer cases identified in the long-term follow-up had a co-testing result showing negative HPV but positive cytology.</p><p><strong>Conclusions: </strong>HPV testing alone, as a single test, is comparable to co-testing in detecting HSIL + up to three years after treatment independently of margin status, and demonstrates a higher specificity. Cytology plays a very limited role in the test of cure analysis and could therefore be omitted.</p>\",\"PeriodicalId\":13568,\"journal\":{\"name\":\"Infectious Agents and Cancer\",\"volume\":\"20 1\",\"pages\":\"59\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392528/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Agents and Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13027-025-00690-y\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Agents and Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13027-025-00690-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
HPV testing alone as a test of cure after treatment with cervical loop excision: a retrospective register-based cohort study.
Background: Women treated with cervical loop electrosurgical excision procedure require follow-up to detect residual or recurrent HSIL+, defined as high-grade squamous intraepithelial lesions, adenocarcinoma in situ or cervical cancer. Currently, co-testing with cytology and human papillomavirus (HPV) analysis is usually recommended. This study investigates whether HPV testing alone is comparable to co-testing in detecting HSIL + up to three years after treatment. Recurrence rates of HSIL + are also presented, with follow-up extending up to 18 years.
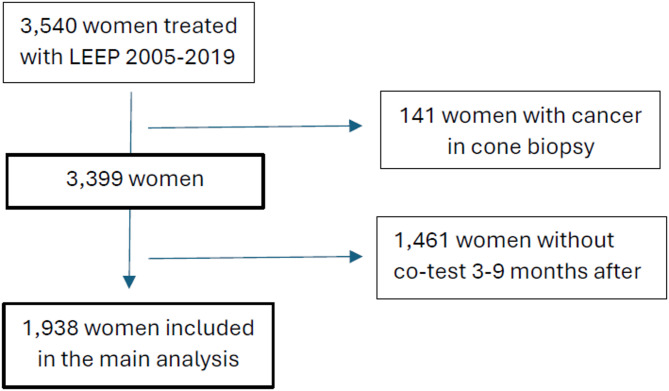
Methods: This retrospective cohort study included all 3,540 women treated with a cervical excision in Uppsala County between 1 January 2005 and 31 December 2019. Women with cancer identified in the cone biopsy were excluded. The main outcome was HSIL + detected within three years of follow-up. Sensitivity, specificity and negative predictive value were calculated for the 1,938 women who had a co-testing result as part of their test of cure. Thus, the analysis for the main outcome could finally be performed on 1,938 out of the total number of 3,540 women. Additionally, long-term data on recurrence and time to HSIL+, along with a separate analysis of results prior to cervical cancer diagnosis, were collected for the whole cohort of 3,399 women.
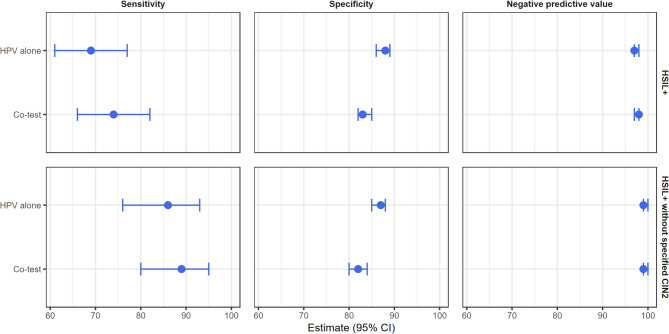
Results: The sensitivity and negative predictive value for detecting HSIL + were 69% and 97% for HPV alone, and 74% and 98% for co-testing, respectively. These differences were not statistically significant. Specificity was higher for HPV alone than for co-testing. The negative predictive value of HPV testing for excluding cervical cancer (n = 5) within three years was 100%. Recurrence rate of HSIL + in the three-year follow up was 8%, and the total recurrence rate of HSIL + with a mean follow-up of nine years was 10%. Mean time to recurrence was 28 months. None of 19 cervical cancer cases identified in the long-term follow-up had a co-testing result showing negative HPV but positive cytology.
Conclusions: HPV testing alone, as a single test, is comparable to co-testing in detecting HSIL + up to three years after treatment independently of margin status, and demonstrates a higher specificity. Cytology plays a very limited role in the test of cure analysis and could therefore be omitted.
期刊介绍:
Infectious Agents and Cancer is an open access, peer-reviewed online journal that encompasses all aspects of basic, clinical, epidemiological and translational research providing an insight into the association between chronic infections and cancer.
The journal welcomes submissions in the pathogen-related cancer areas and other related topics, in particular:
• HPV and anogenital cancers, as well as head and neck cancers;
• EBV and Burkitt lymphoma;
• HCV/HBV and hepatocellular carcinoma as well as lymphoproliferative diseases;
• HHV8 and Kaposi sarcoma;
• HTLV and leukemia;
• Cancers in Low- and Middle-income countries.
The link between infection and cancer has become well established over the past 50 years, and infection-associated cancer contribute up to 16% of cancers in developed countries and 33% in less developed countries.
Preventive vaccines have been developed for only two cancer-causing viruses, highlighting both the opportunity to prevent infection-associated cancers by vaccination and the gaps that remain before vaccines can be developed for other cancer-causing agents. These gaps are due to incomplete understanding of the basic biology, natural history, epidemiology of many of the pathogens that cause cancer, the mechanisms they exploit to cause cancer, and how to interrupt progression to cancer in human populations. Early diagnosis or identification of lesions at high risk of progression represent the current most critical research area of the field supported by recent advances in genomics and proteomics technologies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


