Sebastian M Wingen-Heimann, Christoph Lübbert, Davide Fiore Bavaro, Sina M Hopff
{"title":"美国艰难梭菌感染——67家大型医疗机构中使用非达霉素和万古霉素治疗的患者的比较事件风险分析","authors":"Sebastian M Wingen-Heimann, Christoph Lübbert, Davide Fiore Bavaro, Sina M Hopff","doi":"10.3390/idr17040087","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong><i>Clostridioides difficile</i> infection (CDI) is a major cause of infectious diarrhea in the inpatient and community setting. Real-world data outside the strict environment of randomized controlled trials (RCTs) are needed to improve the quality of evidence. The aim of this study was to compare different clinical outcomes of CDI patients treated with fidaxomicin with those treated with vancomycin using a representative patient population in the United States of America (USA).</p><p><strong>Methods: </strong>Comprehensive real-world data were analyzed for this retrospective observational study, provided by the TriNetX database, an international research network with electronic health records from multiple USA healthcare providers. This includes in- and outpatients treated with fidaxomicin (FDX) or vancomycin (VAN) for CDI between 01/2013 and 12/2023. The following cohorts were compared: (i) patients treated with fidaxomicin within 10 days following CDI diagnosis (FDX group) vs. (ii) patients treated with vancomycin within 10 days following CDI diagnosis (VAN group). Outcomes analysis between the two cohorts was performed after propensity score matching and included event risk and Kaplan-Meier survival analyses for the following concomitant diseases/events occurring during an observational period of 12 months following CDI diagnosis: death, sepsis, candidiasis, infections caused by vancomycin-resistant enterococci, inflammatory bowel disease, cardiovascular disease, psychological disease, central line-associated blood stream infection, surgical site infection, and ventilator-associated pneumonia.</p><p><strong>Results: </strong>Following propensity score matching, 2170 patients were included in the FDX group and VAN groups, respectively. The event risk analysis demonstrated improved outcomes of patients treated with FDX compared to VAN in 6 out of the 10 events that were analyzed. The highest risk ratio (RR) and odds ratio (OR) were found for sepsis (RR: 3.409; OR: 3.635), candidiasis (RR: 2.347; OR: 2.431), and death (RR: 1.710; OR: 1.811). The Kaplan-Meier survival analysis showed an overall survival rate until the end of the 12-month observational period of 87.06% in the FDX group and 78.49% in the VAN group (log-rank <i>p</i> < 0.001).</p><p><strong>Conclusions: </strong>Our comparative event risk analysis demonstrated improved outcomes for patients treated with FDX compared to VAN in most of the observed events and underlines the results of previously conducted RCTs, highlighting the beneficial role of FDX compared to VAN. Further big data analyses from other industrialized countries are needed for comparison with our observations.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 4","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386325/pdf/","citationCount":"0","resultStr":"{\"title\":\"<i>Clostridioides difficile</i> Infection in the United States of America-A Comparative Event Risk Analysis of Patients Treated with Fidaxomicin vs. Vancomycin Across 67 Large Healthcare Providers.\",\"authors\":\"Sebastian M Wingen-Heimann, Christoph Lübbert, Davide Fiore Bavaro, Sina M Hopff\",\"doi\":\"10.3390/idr17040087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/objectives: </strong><i>Clostridioides difficile</i> infection (CDI) is a major cause of infectious diarrhea in the inpatient and community setting. Real-world data outside the strict environment of randomized controlled trials (RCTs) are needed to improve the quality of evidence. The aim of this study was to compare different clinical outcomes of CDI patients treated with fidaxomicin with those treated with vancomycin using a representative patient population in the United States of America (USA).</p><p><strong>Methods: </strong>Comprehensive real-world data were analyzed for this retrospective observational study, provided by the TriNetX database, an international research network with electronic health records from multiple USA healthcare providers. This includes in- and outpatients treated with fidaxomicin (FDX) or vancomycin (VAN) for CDI between 01/2013 and 12/2023. The following cohorts were compared: (i) patients treated with fidaxomicin within 10 days following CDI diagnosis (FDX group) vs. (ii) patients treated with vancomycin within 10 days following CDI diagnosis (VAN group). Outcomes analysis between the two cohorts was performed after propensity score matching and included event risk and Kaplan-Meier survival analyses for the following concomitant diseases/events occurring during an observational period of 12 months following CDI diagnosis: death, sepsis, candidiasis, infections caused by vancomycin-resistant enterococci, inflammatory bowel disease, cardiovascular disease, psychological disease, central line-associated blood stream infection, surgical site infection, and ventilator-associated pneumonia.</p><p><strong>Results: </strong>Following propensity score matching, 2170 patients were included in the FDX group and VAN groups, respectively. The event risk analysis demonstrated improved outcomes of patients treated with FDX compared to VAN in 6 out of the 10 events that were analyzed. The highest risk ratio (RR) and odds ratio (OR) were found for sepsis (RR: 3.409; OR: 3.635), candidiasis (RR: 2.347; OR: 2.431), and death (RR: 1.710; OR: 1.811). The Kaplan-Meier survival analysis showed an overall survival rate until the end of the 12-month observational period of 87.06% in the FDX group and 78.49% in the VAN group (log-rank <i>p</i> < 0.001).</p><p><strong>Conclusions: </strong>Our comparative event risk analysis demonstrated improved outcomes for patients treated with FDX compared to VAN in most of the observed events and underlines the results of previously conducted RCTs, highlighting the beneficial role of FDX compared to VAN. Further big data analyses from other industrialized countries are needed for comparison with our observations.</p>\",\"PeriodicalId\":13579,\"journal\":{\"name\":\"Infectious Disease Reports\",\"volume\":\"17 4\",\"pages\":\"\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386325/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Disease Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/idr17040087\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17040087","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Clostridioides difficile Infection in the United States of America-A Comparative Event Risk Analysis of Patients Treated with Fidaxomicin vs. Vancomycin Across 67 Large Healthcare Providers.
Background/objectives: Clostridioides difficile infection (CDI) is a major cause of infectious diarrhea in the inpatient and community setting. Real-world data outside the strict environment of randomized controlled trials (RCTs) are needed to improve the quality of evidence. The aim of this study was to compare different clinical outcomes of CDI patients treated with fidaxomicin with those treated with vancomycin using a representative patient population in the United States of America (USA).
Methods: Comprehensive real-world data were analyzed for this retrospective observational study, provided by the TriNetX database, an international research network with electronic health records from multiple USA healthcare providers. This includes in- and outpatients treated with fidaxomicin (FDX) or vancomycin (VAN) for CDI between 01/2013 and 12/2023. The following cohorts were compared: (i) patients treated with fidaxomicin within 10 days following CDI diagnosis (FDX group) vs. (ii) patients treated with vancomycin within 10 days following CDI diagnosis (VAN group). Outcomes analysis between the two cohorts was performed after propensity score matching and included event risk and Kaplan-Meier survival analyses for the following concomitant diseases/events occurring during an observational period of 12 months following CDI diagnosis: death, sepsis, candidiasis, infections caused by vancomycin-resistant enterococci, inflammatory bowel disease, cardiovascular disease, psychological disease, central line-associated blood stream infection, surgical site infection, and ventilator-associated pneumonia.
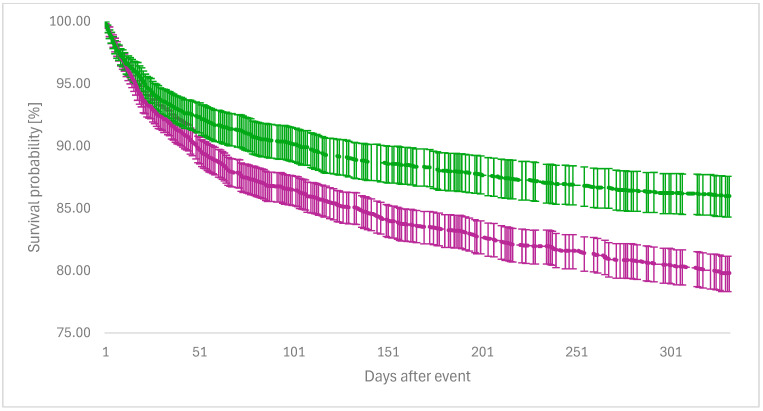
Results: Following propensity score matching, 2170 patients were included in the FDX group and VAN groups, respectively. The event risk analysis demonstrated improved outcomes of patients treated with FDX compared to VAN in 6 out of the 10 events that were analyzed. The highest risk ratio (RR) and odds ratio (OR) were found for sepsis (RR: 3.409; OR: 3.635), candidiasis (RR: 2.347; OR: 2.431), and death (RR: 1.710; OR: 1.811). The Kaplan-Meier survival analysis showed an overall survival rate until the end of the 12-month observational period of 87.06% in the FDX group and 78.49% in the VAN group (log-rank p < 0.001).
Conclusions: Our comparative event risk analysis demonstrated improved outcomes for patients treated with FDX compared to VAN in most of the observed events and underlines the results of previously conducted RCTs, highlighting the beneficial role of FDX compared to VAN. Further big data analyses from other industrialized countries are needed for comparison with our observations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


