{"title":"CT增强诊断小体积cT3a肾细胞癌的准确性及降期至pT1的预测因素分析","authors":"Kensuke Bekku, Kasumi Yoshinaga, Shota Inoue, Yosuke Mitsui, Tomoaki Yamanoi, Tatsushi Kawada, Yusuke Tominaga, Takuya Sadahira, Satoshi Katayama, Takehiro Iwata, Shingo Nishimura, Kohei Edamura, Tomoko Kobayashi, Motoo Araki","doi":"10.21873/invivo.14077","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>This study assessed the accuracy of preoperative contrast-enhanced computed tomography (CECT) scans in staging small-sized, locally advanced (cT3a) renal cell carcinoma (RCC) and identified predictors of pathological downstaging following surgery.</p><p><strong>Patients and methods: </strong>Seventy-six patients who underwent radical nephrectomy for cT3aN0M0 RCC with tumors ≤7 cm were analyzed. Preoperative CECT evaluated features such as venous, peritumoral, or renal sinus fat, and urinary tract invasion, predictive values, and concordance index between radiological and pathological findings were calculated for these categories. The study also examined the impact of clinicopathologic factors on downstaging.</p><p><strong>Results: </strong>Of 76 patients with cT3 RCC, 37% were down-staged to pT1. Down-staged cases had a higher proportion of male patients and non-clear cell carcinoma (86% <i>vs.</i> 58%, 32% <i>vs.</i> 6%; <i>p</i>=0.02, <i>p</i>=0.007, respectively). Multiple cT3a factors were less common in down-staged cases (4% <i>vs.</i> 23%, <i>p</i>=0.04). Non-clear cell carcinoma was significantly associated with downstaging compared to clear cell carcinoma (75% <i>vs.</i> 30%, <i>p</i>=0.006). Multivariate analysis confirmed non-clear cell carcinoma as an independent predictor (odds ratio=8.2, <i>p</i>=0.01). For venous invasion, CECT sensitivity and positive predictive value were high (73.5% and 83.3%, respectively) and the degree of agreement was substantial (κ=0.62).</p><p><strong>Conclusion: </strong>The accuracy of preoperative CECT was acceptable for detecting venous invasion. The downstaging to pT1 occurred in 37% of cT3a RCC cases in the final pathology, with non-clear cell carcinoma being a significant predictor.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 5","pages":"2787-2793"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396049/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of Contrast-enhanced CT in Diagnosing Small-sized cT3a Renal Cell Carcinoma and Analysis of Factors Predicting Downstaging to pT1.\",\"authors\":\"Kensuke Bekku, Kasumi Yoshinaga, Shota Inoue, Yosuke Mitsui, Tomoaki Yamanoi, Tatsushi Kawada, Yusuke Tominaga, Takuya Sadahira, Satoshi Katayama, Takehiro Iwata, Shingo Nishimura, Kohei Edamura, Tomoko Kobayashi, Motoo Araki\",\"doi\":\"10.21873/invivo.14077\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aim: </strong>This study assessed the accuracy of preoperative contrast-enhanced computed tomography (CECT) scans in staging small-sized, locally advanced (cT3a) renal cell carcinoma (RCC) and identified predictors of pathological downstaging following surgery.</p><p><strong>Patients and methods: </strong>Seventy-six patients who underwent radical nephrectomy for cT3aN0M0 RCC with tumors ≤7 cm were analyzed. Preoperative CECT evaluated features such as venous, peritumoral, or renal sinus fat, and urinary tract invasion, predictive values, and concordance index between radiological and pathological findings were calculated for these categories. The study also examined the impact of clinicopathologic factors on downstaging.</p><p><strong>Results: </strong>Of 76 patients with cT3 RCC, 37% were down-staged to pT1. Down-staged cases had a higher proportion of male patients and non-clear cell carcinoma (86% <i>vs.</i> 58%, 32% <i>vs.</i> 6%; <i>p</i>=0.02, <i>p</i>=0.007, respectively). Multiple cT3a factors were less common in down-staged cases (4% <i>vs.</i> 23%, <i>p</i>=0.04). Non-clear cell carcinoma was significantly associated with downstaging compared to clear cell carcinoma (75% <i>vs.</i> 30%, <i>p</i>=0.006). Multivariate analysis confirmed non-clear cell carcinoma as an independent predictor (odds ratio=8.2, <i>p</i>=0.01). For venous invasion, CECT sensitivity and positive predictive value were high (73.5% and 83.3%, respectively) and the degree of agreement was substantial (κ=0.62).</p><p><strong>Conclusion: </strong>The accuracy of preoperative CECT was acceptable for detecting venous invasion. The downstaging to pT1 occurred in 37% of cT3a RCC cases in the final pathology, with non-clear cell carcinoma being a significant predictor.</p>\",\"PeriodicalId\":13364,\"journal\":{\"name\":\"In vivo\",\"volume\":\"39 5\",\"pages\":\"2787-2793\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396049/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"In vivo\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21873/invivo.14077\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.14077","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Accuracy of Contrast-enhanced CT in Diagnosing Small-sized cT3a Renal Cell Carcinoma and Analysis of Factors Predicting Downstaging to pT1.
Background/aim: This study assessed the accuracy of preoperative contrast-enhanced computed tomography (CECT) scans in staging small-sized, locally advanced (cT3a) renal cell carcinoma (RCC) and identified predictors of pathological downstaging following surgery.
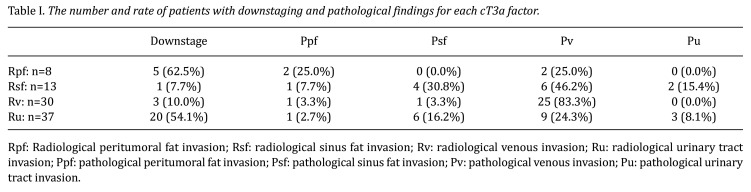
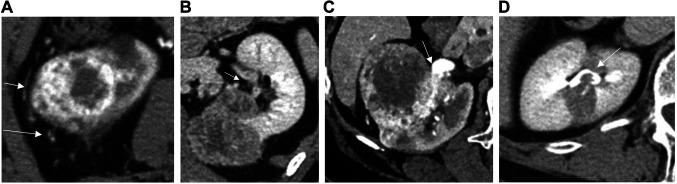
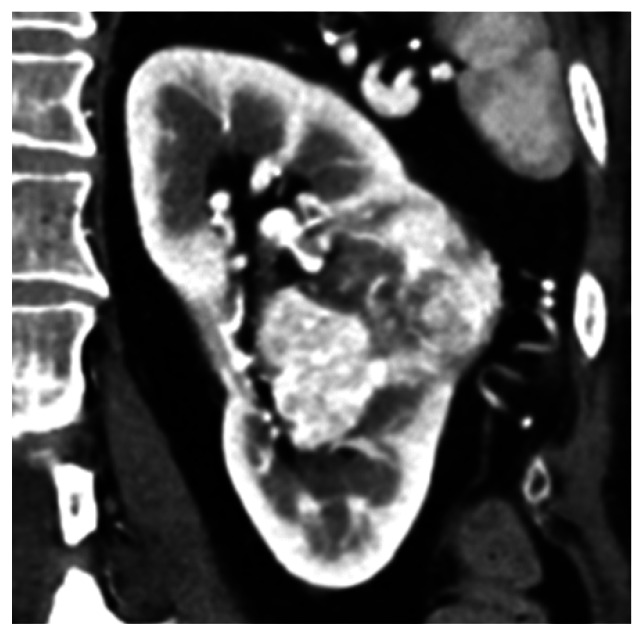
Patients and methods: Seventy-six patients who underwent radical nephrectomy for cT3aN0M0 RCC with tumors ≤7 cm were analyzed. Preoperative CECT evaluated features such as venous, peritumoral, or renal sinus fat, and urinary tract invasion, predictive values, and concordance index between radiological and pathological findings were calculated for these categories. The study also examined the impact of clinicopathologic factors on downstaging.
Results: Of 76 patients with cT3 RCC, 37% were down-staged to pT1. Down-staged cases had a higher proportion of male patients and non-clear cell carcinoma (86% vs. 58%, 32% vs. 6%; p=0.02, p=0.007, respectively). Multiple cT3a factors were less common in down-staged cases (4% vs. 23%, p=0.04). Non-clear cell carcinoma was significantly associated with downstaging compared to clear cell carcinoma (75% vs. 30%, p=0.006). Multivariate analysis confirmed non-clear cell carcinoma as an independent predictor (odds ratio=8.2, p=0.01). For venous invasion, CECT sensitivity and positive predictive value were high (73.5% and 83.3%, respectively) and the degree of agreement was substantial (κ=0.62).
Conclusion: The accuracy of preoperative CECT was acceptable for detecting venous invasion. The downstaging to pT1 occurred in 37% of cT3a RCC cases in the final pathology, with non-clear cell carcinoma being a significant predictor.
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


