{"title":"产后肾皮质坏死的超声边缘征:在三级保健中心的经验。","authors":"Adarsh Kumar, Meenakshi Rajput, Rajesh Kumar, Sanjiv Mahajan, Chirag Jain","doi":"10.25259/IJN_244_2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Kidney biopsy or contrast studies are required to diagnose acute renal cortical necrosis (RCN). Both procedures may be potentially delayed in the postpartum setting. Contrast-enhanced ultrasound (CEUS) is a potential alternative for these patients but remains limited in availability. Due to sparse literature and the rarity of RCN, the role of conventional B-mode ultrasound (USG) in diagnosing RCN remains unexplored.</p><p><strong>Materials and methods: </strong>This retrospective study involved postpartum patients with RCN who underwent kidney biopsy at a tertiary care center. Medical records and B-mode USG kidney images of all 23 patients with postpartum RCN over the past 24 months were retrieved. Gray-scale B-mode USG images of the kidney were assessed for size, presence of sonographic hypoechoic rim, USG kidney timing, echogenicity, and cortico-medullary differentiation.</p><p><strong>Results: </strong>Among the 23 patients, sonographic hypoechoic rim was observed in 6 patients (26.1%). USG kidney timing ranged from 1.1 to 8 weeks, and kidney length varied from 9.0 to 10.8 cm. There were significant differences in mean USG kidney timing and mean kidney length between patients with and without hypoechoic rim (<i>P</i>= 0.020 and <i>P</i>= 0.036, respectively). The mean USG kidney timing was notably earlier in patients with sonographic rim signs than those without sonographic rim signs (2.5 ± 0.77 weeks and 4.81 ± 2.17 weeks, respectively).</p><p><strong>Conclusion: </strong>Despite its lower sensitivity, the sonographic rim sign is an important diagnostic feature of postpartum renal cortical necrosis. In point-of-care ultrasonography, it should be looked for early in the disease course, especially in cases of postpartum anuric acute kidney injury.</p>","PeriodicalId":13359,"journal":{"name":"Indian Journal of Nephrology","volume":"35 4","pages":"520-523"},"PeriodicalIF":0.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392187/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sono-graphic Rim Sign in Postpartum Renal Cortical Necrosis: Experience at a Tertiary Care Centre.\",\"authors\":\"Adarsh Kumar, Meenakshi Rajput, Rajesh Kumar, Sanjiv Mahajan, Chirag Jain\",\"doi\":\"10.25259/IJN_244_2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Kidney biopsy or contrast studies are required to diagnose acute renal cortical necrosis (RCN). Both procedures may be potentially delayed in the postpartum setting. Contrast-enhanced ultrasound (CEUS) is a potential alternative for these patients but remains limited in availability. Due to sparse literature and the rarity of RCN, the role of conventional B-mode ultrasound (USG) in diagnosing RCN remains unexplored.</p><p><strong>Materials and methods: </strong>This retrospective study involved postpartum patients with RCN who underwent kidney biopsy at a tertiary care center. Medical records and B-mode USG kidney images of all 23 patients with postpartum RCN over the past 24 months were retrieved. Gray-scale B-mode USG images of the kidney were assessed for size, presence of sonographic hypoechoic rim, USG kidney timing, echogenicity, and cortico-medullary differentiation.</p><p><strong>Results: </strong>Among the 23 patients, sonographic hypoechoic rim was observed in 6 patients (26.1%). USG kidney timing ranged from 1.1 to 8 weeks, and kidney length varied from 9.0 to 10.8 cm. There were significant differences in mean USG kidney timing and mean kidney length between patients with and without hypoechoic rim (<i>P</i>= 0.020 and <i>P</i>= 0.036, respectively). The mean USG kidney timing was notably earlier in patients with sonographic rim signs than those without sonographic rim signs (2.5 ± 0.77 weeks and 4.81 ± 2.17 weeks, respectively).</p><p><strong>Conclusion: </strong>Despite its lower sensitivity, the sonographic rim sign is an important diagnostic feature of postpartum renal cortical necrosis. In point-of-care ultrasonography, it should be looked for early in the disease course, especially in cases of postpartum anuric acute kidney injury.</p>\",\"PeriodicalId\":13359,\"journal\":{\"name\":\"Indian Journal of Nephrology\",\"volume\":\"35 4\",\"pages\":\"520-523\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392187/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Journal of Nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/IJN_244_2024\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/IJN_244_2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/5 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Sono-graphic Rim Sign in Postpartum Renal Cortical Necrosis: Experience at a Tertiary Care Centre.
Background: Kidney biopsy or contrast studies are required to diagnose acute renal cortical necrosis (RCN). Both procedures may be potentially delayed in the postpartum setting. Contrast-enhanced ultrasound (CEUS) is a potential alternative for these patients but remains limited in availability. Due to sparse literature and the rarity of RCN, the role of conventional B-mode ultrasound (USG) in diagnosing RCN remains unexplored.
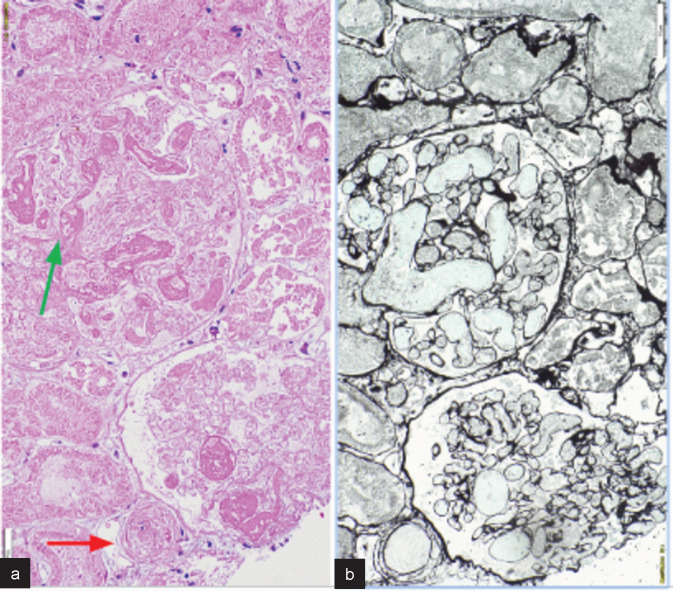
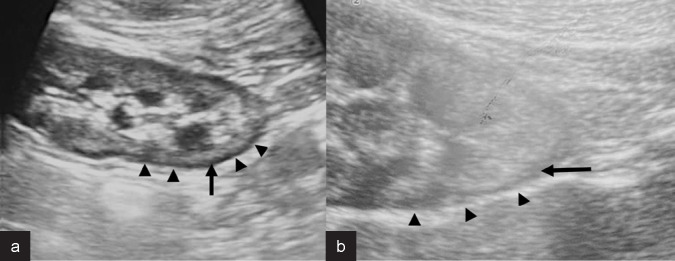
Materials and methods: This retrospective study involved postpartum patients with RCN who underwent kidney biopsy at a tertiary care center. Medical records and B-mode USG kidney images of all 23 patients with postpartum RCN over the past 24 months were retrieved. Gray-scale B-mode USG images of the kidney were assessed for size, presence of sonographic hypoechoic rim, USG kidney timing, echogenicity, and cortico-medullary differentiation.
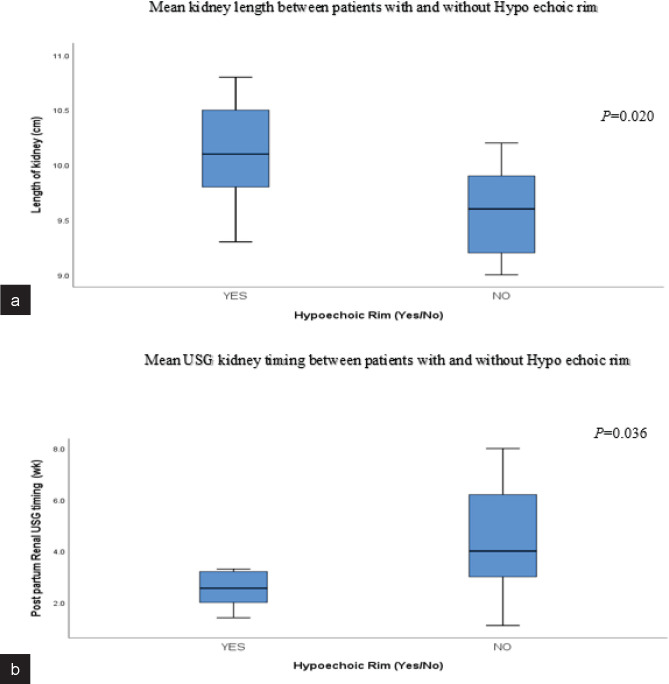
Results: Among the 23 patients, sonographic hypoechoic rim was observed in 6 patients (26.1%). USG kidney timing ranged from 1.1 to 8 weeks, and kidney length varied from 9.0 to 10.8 cm. There were significant differences in mean USG kidney timing and mean kidney length between patients with and without hypoechoic rim (P= 0.020 and P= 0.036, respectively). The mean USG kidney timing was notably earlier in patients with sonographic rim signs than those without sonographic rim signs (2.5 ± 0.77 weeks and 4.81 ± 2.17 weeks, respectively).
Conclusion: Despite its lower sensitivity, the sonographic rim sign is an important diagnostic feature of postpartum renal cortical necrosis. In point-of-care ultrasonography, it should be looked for early in the disease course, especially in cases of postpartum anuric acute kidney injury.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


