Xinmin Duan, Xiaojing Song, Wei Lyu, Yanling Li, Jing Tang, Wei Cao, Yang Han, Taisheng Li
{"title":"基于nnrti方案的HIV低水平病毒血症与随后的病毒学失败无关:中国的一项多中心回顾性研究","authors":"Xinmin Duan, Xiaojing Song, Wei Lyu, Yanling Li, Jing Tang, Wei Cao, Yang Han, Taisheng Li","doi":"10.2147/IDR.S533871","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The long-term impact of low-level viremia (LLV), defined as two consecutive viral loads (VL) of <200 copies/mL, on virological failure remains unclear. This study aimed to investigate the association between viremia patterns and virological failure in people living with HIV (PLWH) in China who predominantly received non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapies.</p><p><strong>Methods: </strong>Data from six HIV-infected cohorts in China were analyzed. Adult antiretroviral therapy (ART)-naïve patients were included. Patients were excluded if they received less than 24 weeks of ART, had fewer than two documented VL and CD4+ T cell count, initiated ART during the acute infection stage, or had a follow-up duration of less than 48 weeks. All patients were stratified according to virological suppression (VS), virological blips (VB), or LLV. Cox regression analysis was used to evaluate the association between virological failure and patterns of viremia. Genotypic drug resistance mutations were compared at baseline and during LLV.</p><p><strong>Results: </strong>Among the 1532 patients, 374 (24.4%) had blips and 166 (10.8%) had LLV. The LLV group had a higher baseline viral load and lower CD4<sup>+</sup> T cell count. Approximately 90% of patients received NNRTI-based regimens. In the adjusted Cox regression, neither the blip nor LLV groups demonstrated a significantly increased risk of virological failure compared to the VS group (Blip, adjusted HR = 0.5 [95% CI: 0.2-1.2], <i>p</i> = 0.116; LLV, aHR = 0.7 [95% CI: 0.3-1.9], <i>p</i> = 0.474). Among the 17 patients who successfully underwent sequencing, three (17.6%) developed new drug resistance mutations, but none experienced virological failure.</p><p><strong>Conclusion: </strong>Neither blip nor LLV were significantly associated with an increased risk of virological failure in China. Emerging drug resistance mutations in LLV are rare and do not correlate with subsequent virological failures. Further research is needed to understand the clinical significance of these patterns of viremia.</p>","PeriodicalId":13577,"journal":{"name":"Infection and Drug Resistance","volume":"18 ","pages":"4373-4384"},"PeriodicalIF":2.9000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399107/pdf/","citationCount":"0","resultStr":"{\"title\":\"HIV Low-Level Viremia is Not Related to Subsequent Virological Failure Under NNRTI-Based Regimens: A Multicenter Retrospective Study in China.\",\"authors\":\"Xinmin Duan, Xiaojing Song, Wei Lyu, Yanling Li, Jing Tang, Wei Cao, Yang Han, Taisheng Li\",\"doi\":\"10.2147/IDR.S533871\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The long-term impact of low-level viremia (LLV), defined as two consecutive viral loads (VL) of <200 copies/mL, on virological failure remains unclear. This study aimed to investigate the association between viremia patterns and virological failure in people living with HIV (PLWH) in China who predominantly received non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapies.</p><p><strong>Methods: </strong>Data from six HIV-infected cohorts in China were analyzed. Adult antiretroviral therapy (ART)-naïve patients were included. Patients were excluded if they received less than 24 weeks of ART, had fewer than two documented VL and CD4+ T cell count, initiated ART during the acute infection stage, or had a follow-up duration of less than 48 weeks. All patients were stratified according to virological suppression (VS), virological blips (VB), or LLV. Cox regression analysis was used to evaluate the association between virological failure and patterns of viremia. Genotypic drug resistance mutations were compared at baseline and during LLV.</p><p><strong>Results: </strong>Among the 1532 patients, 374 (24.4%) had blips and 166 (10.8%) had LLV. The LLV group had a higher baseline viral load and lower CD4<sup>+</sup> T cell count. Approximately 90% of patients received NNRTI-based regimens. In the adjusted Cox regression, neither the blip nor LLV groups demonstrated a significantly increased risk of virological failure compared to the VS group (Blip, adjusted HR = 0.5 [95% CI: 0.2-1.2], <i>p</i> = 0.116; LLV, aHR = 0.7 [95% CI: 0.3-1.9], <i>p</i> = 0.474). Among the 17 patients who successfully underwent sequencing, three (17.6%) developed new drug resistance mutations, but none experienced virological failure.</p><p><strong>Conclusion: </strong>Neither blip nor LLV were significantly associated with an increased risk of virological failure in China. Emerging drug resistance mutations in LLV are rare and do not correlate with subsequent virological failures. Further research is needed to understand the clinical significance of these patterns of viremia.</p>\",\"PeriodicalId\":13577,\"journal\":{\"name\":\"Infection and Drug Resistance\",\"volume\":\"18 \",\"pages\":\"4373-4384\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399107/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infection and Drug Resistance\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/IDR.S533871\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection and Drug Resistance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/IDR.S533871","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
背景:低水平病毒血症(LLV)的长期影响,定义为两个连续病毒载量(VL)的方法:分析来自中国6个hiv感染队列的数据。纳入成人抗逆转录病毒治疗(ART)-naïve患者。如果患者接受的抗逆转录病毒治疗少于24周,记录的VL和CD4+ T细胞计数少于2个,在急性感染阶段开始抗逆转录病毒治疗,或随访时间少于48周,则排除患者。所有患者根据病毒学抑制(VS)、病毒学亮点(VB)或LLV进行分层。采用Cox回归分析评估病毒学失败与病毒血症模式之间的关系。在基线和LLV期间比较基因型耐药突变。结果:1532例患者中,374例(24.4%)有小肿块,166例(10.8%)有LLV。LLV组有较高的基线病毒载量和较低的CD4+ T细胞计数。大约90%的患者接受了基于nnrti的治疗方案。在校正Cox回归中,与VS组相比,blip组和LLV组均未表现出明显的病毒学失败风险增加(blip组,校正HR = 0.5 [95% CI: 0.2-1.2], p = 0.116; LLV组,aHR = 0.7 [95% CI: 0.3-1.9], p = 0.474)。在成功测序的17例患者中,3例(17.6%)出现了新的耐药突变,但没有出现病毒学失败。结论:在中国,blip和LLV与病毒学失败风险增加均无显著相关性。LLV中出现的耐药突变是罕见的,与随后的病毒学失败无关。需要进一步的研究来了解这些病毒血症的临床意义。
HIV Low-Level Viremia is Not Related to Subsequent Virological Failure Under NNRTI-Based Regimens: A Multicenter Retrospective Study in China.
Background: The long-term impact of low-level viremia (LLV), defined as two consecutive viral loads (VL) of <200 copies/mL, on virological failure remains unclear. This study aimed to investigate the association between viremia patterns and virological failure in people living with HIV (PLWH) in China who predominantly received non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapies.
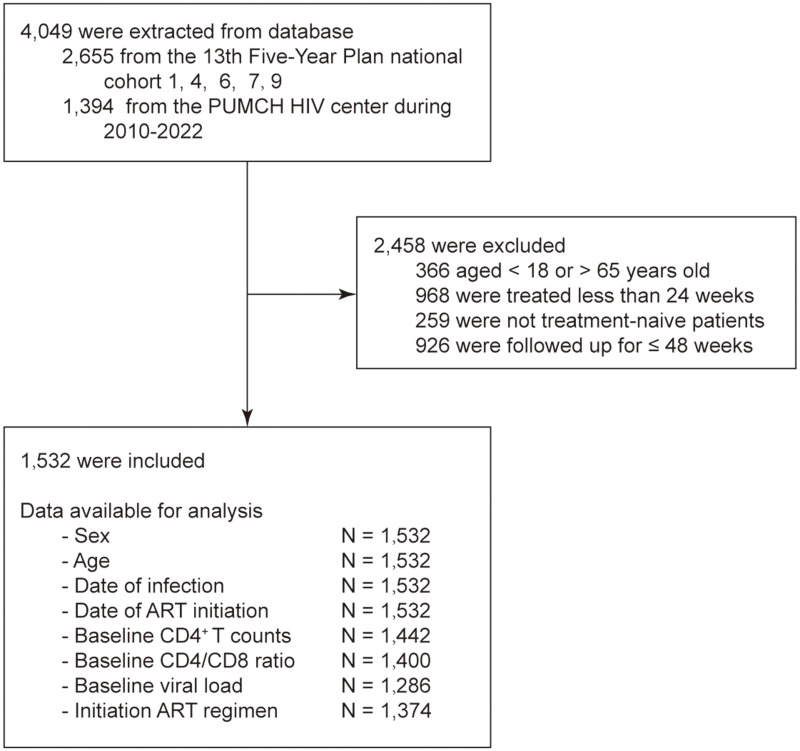
Methods: Data from six HIV-infected cohorts in China were analyzed. Adult antiretroviral therapy (ART)-naïve patients were included. Patients were excluded if they received less than 24 weeks of ART, had fewer than two documented VL and CD4+ T cell count, initiated ART during the acute infection stage, or had a follow-up duration of less than 48 weeks. All patients were stratified according to virological suppression (VS), virological blips (VB), or LLV. Cox regression analysis was used to evaluate the association between virological failure and patterns of viremia. Genotypic drug resistance mutations were compared at baseline and during LLV.
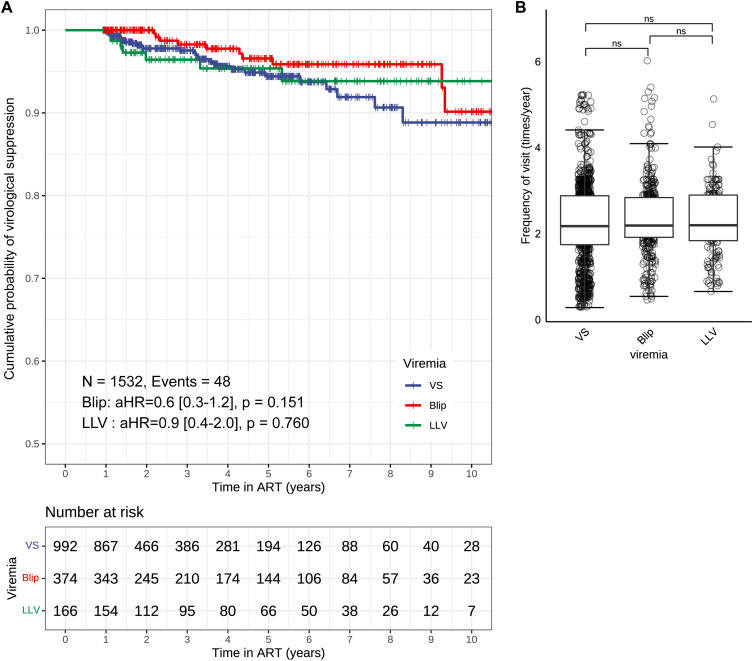
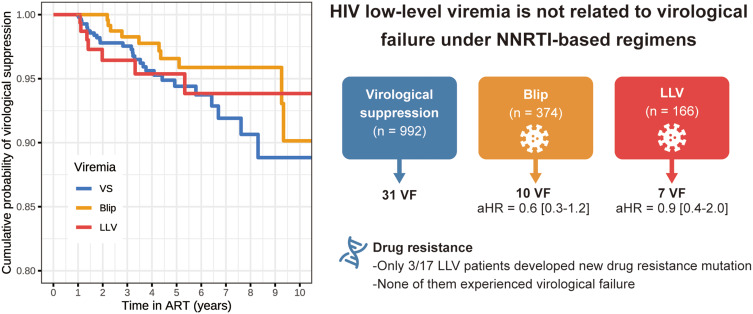
Results: Among the 1532 patients, 374 (24.4%) had blips and 166 (10.8%) had LLV. The LLV group had a higher baseline viral load and lower CD4+ T cell count. Approximately 90% of patients received NNRTI-based regimens. In the adjusted Cox regression, neither the blip nor LLV groups demonstrated a significantly increased risk of virological failure compared to the VS group (Blip, adjusted HR = 0.5 [95% CI: 0.2-1.2], p = 0.116; LLV, aHR = 0.7 [95% CI: 0.3-1.9], p = 0.474). Among the 17 patients who successfully underwent sequencing, three (17.6%) developed new drug resistance mutations, but none experienced virological failure.
Conclusion: Neither blip nor LLV were significantly associated with an increased risk of virological failure in China. Emerging drug resistance mutations in LLV are rare and do not correlate with subsequent virological failures. Further research is needed to understand the clinical significance of these patterns of viremia.
期刊介绍:
About Journal
Editors
Peer Reviewers
Articles
Article Publishing Charges
Aims and Scope
Call For Papers
ISSN: 1178-6973
Editor-in-Chief: Professor Suresh Antony
An international, peer-reviewed, open access journal that focuses on the optimal treatment of infection (bacterial, fungal and viral) and the development and institution of preventative strategies to minimize the development and spread of resistance.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


