Kavitha Athota, Smitha S Prabhu, Niranjana Gopinathan
{"title":"外阴瘤变的不同面貌。","authors":"Kavitha Athota, Smitha S Prabhu, Niranjana Gopinathan","doi":"10.4103/idoj.idoj_911_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>Vulvar neoplasia is on the rise and patients often present to dermatologists with lesions of varying morphology associated with pruritus, burning sensation, or pain. Early diagnosis results in an early treatment and improved quality of life. Differentiating vulvar neoplasia and intraepithelial malignancies from benign and inflammatory conditions is imperative. Histopathology and immunohistochemistry (IHC) are helpful. Herein, we report eight women who presented with varying features. Five of them had predisposing factors- four had lichen sclerosus, and one was human immunodeficiency virus (HIV) positive. All women were diagnosed and treated promptly. Vulvar malignancies encompass both invasive vulvar squamous cell carcinoma (SCC) and its precursors, as well as other less common forms like melanoma, basal cell carcinoma, and extramammary Paget's disease. Vulvar SCC contributes to 80%-90% of vulvar malignancies. It's precursor lesions, vulvar intraepithelial neoplasia (VIN), are now classified as differentiated VIN (dVIN), low-grade squamous intraepithelial neoplasias (LSIL), and high grade squamous intraepithelial neoplasias (HSIL). VIN are of varying morphology and are diagnosed by histopathology and IHC. Dermoscopy of VIN is still evolving. Herein, we also describe the dermoscopic features of lesions encountered. Treatment is resection, wherever possible.</p>","PeriodicalId":13335,"journal":{"name":"Indian Dermatology Online Journal","volume":"16 5","pages":"773-777"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12419734/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Varying Faces of Vulvar Neoplasia.\",\"authors\":\"Kavitha Athota, Smitha S Prabhu, Niranjana Gopinathan\",\"doi\":\"10.4103/idoj.idoj_911_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>Vulvar neoplasia is on the rise and patients often present to dermatologists with lesions of varying morphology associated with pruritus, burning sensation, or pain. Early diagnosis results in an early treatment and improved quality of life. Differentiating vulvar neoplasia and intraepithelial malignancies from benign and inflammatory conditions is imperative. Histopathology and immunohistochemistry (IHC) are helpful. Herein, we report eight women who presented with varying features. Five of them had predisposing factors- four had lichen sclerosus, and one was human immunodeficiency virus (HIV) positive. All women were diagnosed and treated promptly. Vulvar malignancies encompass both invasive vulvar squamous cell carcinoma (SCC) and its precursors, as well as other less common forms like melanoma, basal cell carcinoma, and extramammary Paget's disease. Vulvar SCC contributes to 80%-90% of vulvar malignancies. It's precursor lesions, vulvar intraepithelial neoplasia (VIN), are now classified as differentiated VIN (dVIN), low-grade squamous intraepithelial neoplasias (LSIL), and high grade squamous intraepithelial neoplasias (HSIL). VIN are of varying morphology and are diagnosed by histopathology and IHC. Dermoscopy of VIN is still evolving. Herein, we also describe the dermoscopic features of lesions encountered. Treatment is resection, wherever possible.</p>\",\"PeriodicalId\":13335,\"journal\":{\"name\":\"Indian Dermatology Online Journal\",\"volume\":\"16 5\",\"pages\":\"773-777\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12419734/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Dermatology Online Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/idoj.idoj_911_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Dermatology Online Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/idoj.idoj_911_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
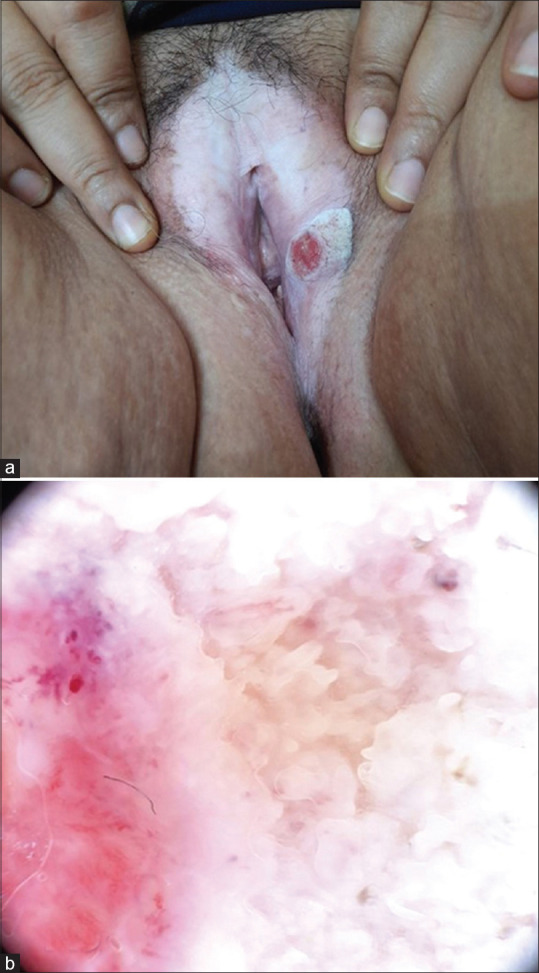
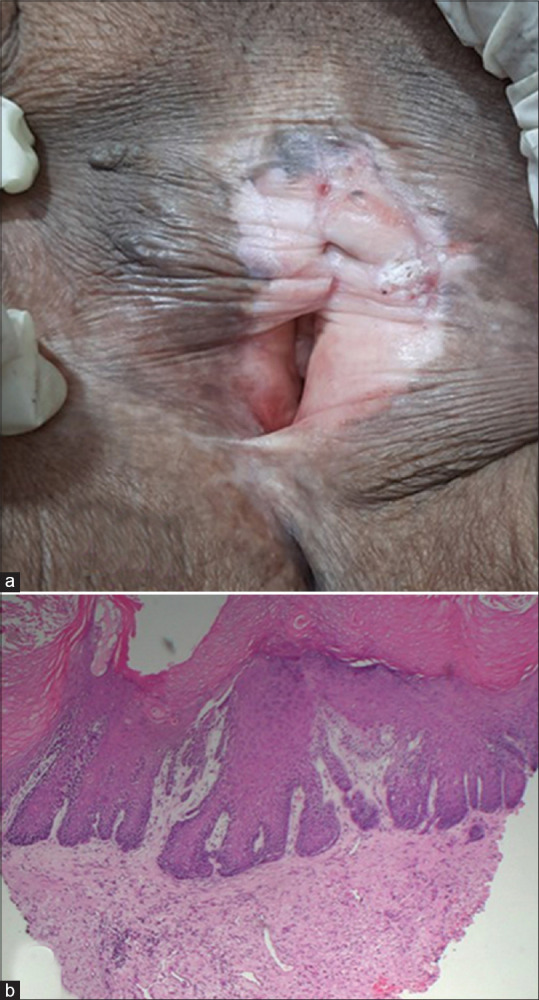
Abstract: Vulvar neoplasia is on the rise and patients often present to dermatologists with lesions of varying morphology associated with pruritus, burning sensation, or pain. Early diagnosis results in an early treatment and improved quality of life. Differentiating vulvar neoplasia and intraepithelial malignancies from benign and inflammatory conditions is imperative. Histopathology and immunohistochemistry (IHC) are helpful. Herein, we report eight women who presented with varying features. Five of them had predisposing factors- four had lichen sclerosus, and one was human immunodeficiency virus (HIV) positive. All women were diagnosed and treated promptly. Vulvar malignancies encompass both invasive vulvar squamous cell carcinoma (SCC) and its precursors, as well as other less common forms like melanoma, basal cell carcinoma, and extramammary Paget's disease. Vulvar SCC contributes to 80%-90% of vulvar malignancies. It's precursor lesions, vulvar intraepithelial neoplasia (VIN), are now classified as differentiated VIN (dVIN), low-grade squamous intraepithelial neoplasias (LSIL), and high grade squamous intraepithelial neoplasias (HSIL). VIN are of varying morphology and are diagnosed by histopathology and IHC. Dermoscopy of VIN is still evolving. Herein, we also describe the dermoscopic features of lesions encountered. Treatment is resection, wherever possible.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


