Daphne Remulla, Kimberly P Woo, William C Bennett, Alvaro Carvalho, Brianna L Slatnick, Marisa H Blackman, Kimberly S Miles, Clayton C Petro, Lucas R Beffa, Ajita S Prabhu, Michael J Rosen, David M Krpata, Benjamin T Miller
{"title":"经腹释放法预测腹疝修补术中筋膜不闭合:危险因素、临床结果和手术计划的意义。","authors":"Daphne Remulla, Kimberly P Woo, William C Bennett, Alvaro Carvalho, Brianna L Slatnick, Marisa H Blackman, Kimberly S Miles, Clayton C Petro, Lucas R Beffa, Ajita S Prabhu, Michael J Rosen, David M Krpata, Benjamin T Miller","doi":"10.1007/s10029-025-03455-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Posterior components separation with transversus abdominis release (TAR) reduces tension on the anterior and posterior fascial elements in complex ventral hernia repairs, but its use does not ensure complete fascial closure. This study evaluates the relationship between hernia size and anterior fascial closure success rates following TAR and identifies predictive factors for non-closure.</p><p><strong>Methods: </strong>We retrospectively analyzed 1,677 patients who underwent open ventral hernia repair with TAR and synthetic mesh placement at a single institution from 2014 to 2023. The primary outcome was the rate of overall anterior fascial closure after TAR. Secondary outcomes included the association of hernia size with fascial closure, predictors of fascial closure and wound morbidity.</p><p><strong>Results: </strong>The overall fascial closure rate was 93.9% (n = 1,574). Hernia width independently predicted fascial closure success, with reduced odds for widths of 15-20 cm (OR 0.39, p = 0.017) and > 20 cm (OR 0.05, p < 0.001), relative to hernias < 15 cm. History of open abdomen (OR 0.33, p < 0.001) and higher ASA classification (OR 0.39, p = 0.042) were associated with non-closure. Fascial non-closure was associated with increased wound morbidity (p < 0.05), while closure independently reduced odds of one-year surgical site infection (SSI) (OR 0.13; p < 0.001) and surgical site infections and occurrences requiring procedural intervention (SSI/O PI) (OR 0.52; p = 0.001).</p><p><strong>Conclusions: </strong>While excellent overall fascial closure rates were achieved among patients undergoing TAR, specific patient and hernia characteristics significantly impact success. These findings establish a reference point for closure rates by hernia width and identify high-risk populations who may benefit from preoperative adjunctive interventions.</p>","PeriodicalId":13168,"journal":{"name":"Hernia","volume":"29 1","pages":"268"},"PeriodicalIF":2.4000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398447/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predicting fascial non-closure in ventral hernia repair with transversus abdominis release: risk factors, clinical outcomes, and implications for surgical planning.\",\"authors\":\"Daphne Remulla, Kimberly P Woo, William C Bennett, Alvaro Carvalho, Brianna L Slatnick, Marisa H Blackman, Kimberly S Miles, Clayton C Petro, Lucas R Beffa, Ajita S Prabhu, Michael J Rosen, David M Krpata, Benjamin T Miller\",\"doi\":\"10.1007/s10029-025-03455-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Posterior components separation with transversus abdominis release (TAR) reduces tension on the anterior and posterior fascial elements in complex ventral hernia repairs, but its use does not ensure complete fascial closure. This study evaluates the relationship between hernia size and anterior fascial closure success rates following TAR and identifies predictive factors for non-closure.</p><p><strong>Methods: </strong>We retrospectively analyzed 1,677 patients who underwent open ventral hernia repair with TAR and synthetic mesh placement at a single institution from 2014 to 2023. The primary outcome was the rate of overall anterior fascial closure after TAR. Secondary outcomes included the association of hernia size with fascial closure, predictors of fascial closure and wound morbidity.</p><p><strong>Results: </strong>The overall fascial closure rate was 93.9% (n = 1,574). Hernia width independently predicted fascial closure success, with reduced odds for widths of 15-20 cm (OR 0.39, p = 0.017) and > 20 cm (OR 0.05, p < 0.001), relative to hernias < 15 cm. History of open abdomen (OR 0.33, p < 0.001) and higher ASA classification (OR 0.39, p = 0.042) were associated with non-closure. Fascial non-closure was associated with increased wound morbidity (p < 0.05), while closure independently reduced odds of one-year surgical site infection (SSI) (OR 0.13; p < 0.001) and surgical site infections and occurrences requiring procedural intervention (SSI/O PI) (OR 0.52; p = 0.001).</p><p><strong>Conclusions: </strong>While excellent overall fascial closure rates were achieved among patients undergoing TAR, specific patient and hernia characteristics significantly impact success. These findings establish a reference point for closure rates by hernia width and identify high-risk populations who may benefit from preoperative adjunctive interventions.</p>\",\"PeriodicalId\":13168,\"journal\":{\"name\":\"Hernia\",\"volume\":\"29 1\",\"pages\":\"268\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398447/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hernia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10029-025-03455-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hernia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10029-025-03455-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
背景:在复杂的腹疝修补中,经腹释放(TAR)分离后成分可减少前后筋膜成分的张力,但其使用并不能确保完全的筋膜闭合。本研究评估了TAR术后疝大小与前筋膜闭合成功率之间的关系,并确定了未闭合的预测因素。方法:我们回顾性分析了2014年至2023年在同一机构接受TAR和合成补片放置的开放腹疝修补术的1,677例患者。主要结果是TAR术后整体前筋膜闭合率。次要结局包括疝气大小与筋膜闭合的关系、筋膜闭合的预测因素和伤口的发病率。结果:总筋膜闭合率为93.9% (n = 1574)。疝宽度独立预测筋膜闭合成功,宽度为15-20 cm (OR 0.39, p = 0.017)和宽度为100 -20 cm (OR 0.05, p)的患者的几率降低。结论:虽然接受TAR的患者总体筋膜闭合率很高,但特定的患者和疝特征显著影响成功。这些发现建立了疝气宽度闭合率的参考点,并确定了可能受益于术前辅助干预的高危人群。
Predicting fascial non-closure in ventral hernia repair with transversus abdominis release: risk factors, clinical outcomes, and implications for surgical planning.
Background: Posterior components separation with transversus abdominis release (TAR) reduces tension on the anterior and posterior fascial elements in complex ventral hernia repairs, but its use does not ensure complete fascial closure. This study evaluates the relationship between hernia size and anterior fascial closure success rates following TAR and identifies predictive factors for non-closure.
Methods: We retrospectively analyzed 1,677 patients who underwent open ventral hernia repair with TAR and synthetic mesh placement at a single institution from 2014 to 2023. The primary outcome was the rate of overall anterior fascial closure after TAR. Secondary outcomes included the association of hernia size with fascial closure, predictors of fascial closure and wound morbidity.
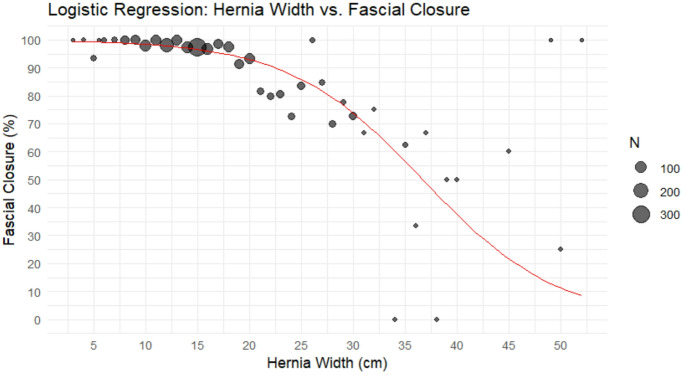
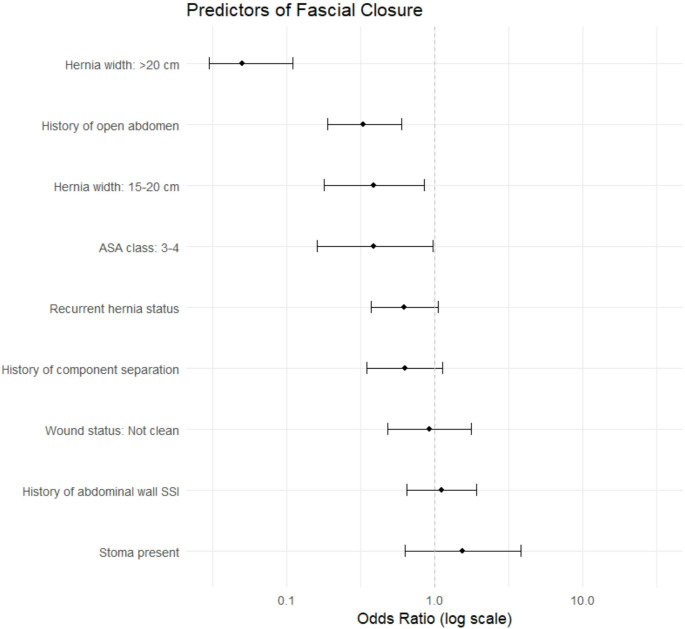
Results: The overall fascial closure rate was 93.9% (n = 1,574). Hernia width independently predicted fascial closure success, with reduced odds for widths of 15-20 cm (OR 0.39, p = 0.017) and > 20 cm (OR 0.05, p < 0.001), relative to hernias < 15 cm. History of open abdomen (OR 0.33, p < 0.001) and higher ASA classification (OR 0.39, p = 0.042) were associated with non-closure. Fascial non-closure was associated with increased wound morbidity (p < 0.05), while closure independently reduced odds of one-year surgical site infection (SSI) (OR 0.13; p < 0.001) and surgical site infections and occurrences requiring procedural intervention (SSI/O PI) (OR 0.52; p = 0.001).
Conclusions: While excellent overall fascial closure rates were achieved among patients undergoing TAR, specific patient and hernia characteristics significantly impact success. These findings establish a reference point for closure rates by hernia width and identify high-risk populations who may benefit from preoperative adjunctive interventions.
期刊介绍:
Hernia was founded in 1997 by Jean P. Chevrel with the purpose of promoting clinical studies and basic research as they apply to groin hernias and the abdominal wall . Since that time, a true revolution in the field of hernia studies has transformed the field from a ”simple” disease to one that is very specialized. While the majority of surgeries for primary inguinal and abdominal wall hernia are performed in hospitals worldwide, complex situations such as multi recurrences, complications, abdominal wall reconstructions and others are being studied and treated in specialist centers. As a result, major institutions and societies are creating specific parameters and criteria to better address the complexities of hernia surgery.
Hernia is a journal written by surgeons who have made abdominal wall surgery their specific field of interest, but we will consider publishing content from any surgeon who wishes to improve the science of this field. The Journal aims to ensure that hernia surgery is safer and easier for surgeons as well as patients, and provides a forum to all surgeons in the exchange of new ideas, results, and important research that is the basis of professional activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


