Bradley Woolfenden, Christian Cawley, Deirdre Ward
{"title":"顽固性心肌炎的重新诊断1例。","authors":"Bradley Woolfenden, Christian Cawley, Deirdre Ward","doi":"10.1093/ehjcr/ytaf379","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Myocarditis typically presents with chest pain, a raised troponin and is associated with late gadolinium enhancement (LGE) on cardiac magnetic resonance imaging (CMR). However, non-resolution of symptoms despite treatment should raise cause for concern that an alternative diagnosis may be present.</p><p><strong>Case summary: </strong>A 17-year-old gentleman with a background history of developmental delay, gastrointestinal motility issues, retractile testes, and patellar dislocation presented to our emergency department with chest pain. Investigations revealed static mildly elevated troponin T. An electrocardiogram and transthoracic echocardiogram were both unremarkable. CMR revealed sub-endocardial and mid-wall LGE. He was treated as myocarditis with steroids and colchicine, however symptoms persisted and repeat CMR reported progressive LGE. The diagnosis of myocarditis was reconsidered given an atypical presentation and taking into account his past medical history, and so a whole gene exome was performed. This revealed a dual diagnosis of Klinefelter's Syndrome and a mutation in the dystrophin gene located on the X chromosome.</p><p><strong>Discussion: </strong>In this case, an interplay between Klinefelter's Syndrome and Muscular Dystrophy is demonstrated, potentially protecting our patient against a more aggressive Duchenne phenotype of muscular dystrophy. Upon non-resolution of symptoms, re-evaluating his presentation, investigations and taking into account his background multi-system medical history lead us to performing the genetic testing which revealed the correct diagnosis.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf379"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398724/pdf/","citationCount":"0","resultStr":"{\"title\":\"A reconsidered diagnosis in an unresolving myocarditis-a case report.\",\"authors\":\"Bradley Woolfenden, Christian Cawley, Deirdre Ward\",\"doi\":\"10.1093/ehjcr/ytaf379\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Myocarditis typically presents with chest pain, a raised troponin and is associated with late gadolinium enhancement (LGE) on cardiac magnetic resonance imaging (CMR). However, non-resolution of symptoms despite treatment should raise cause for concern that an alternative diagnosis may be present.</p><p><strong>Case summary: </strong>A 17-year-old gentleman with a background history of developmental delay, gastrointestinal motility issues, retractile testes, and patellar dislocation presented to our emergency department with chest pain. Investigations revealed static mildly elevated troponin T. An electrocardiogram and transthoracic echocardiogram were both unremarkable. CMR revealed sub-endocardial and mid-wall LGE. He was treated as myocarditis with steroids and colchicine, however symptoms persisted and repeat CMR reported progressive LGE. The diagnosis of myocarditis was reconsidered given an atypical presentation and taking into account his past medical history, and so a whole gene exome was performed. This revealed a dual diagnosis of Klinefelter's Syndrome and a mutation in the dystrophin gene located on the X chromosome.</p><p><strong>Discussion: </strong>In this case, an interplay between Klinefelter's Syndrome and Muscular Dystrophy is demonstrated, potentially protecting our patient against a more aggressive Duchenne phenotype of muscular dystrophy. Upon non-resolution of symptoms, re-evaluating his presentation, investigations and taking into account his background multi-system medical history lead us to performing the genetic testing which revealed the correct diagnosis.</p>\",\"PeriodicalId\":11910,\"journal\":{\"name\":\"European Heart Journal: Case Reports\",\"volume\":\"9 9\",\"pages\":\"ytaf379\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398724/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal: Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcr/ytaf379\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf379","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A reconsidered diagnosis in an unresolving myocarditis-a case report.
Background: Myocarditis typically presents with chest pain, a raised troponin and is associated with late gadolinium enhancement (LGE) on cardiac magnetic resonance imaging (CMR). However, non-resolution of symptoms despite treatment should raise cause for concern that an alternative diagnosis may be present.
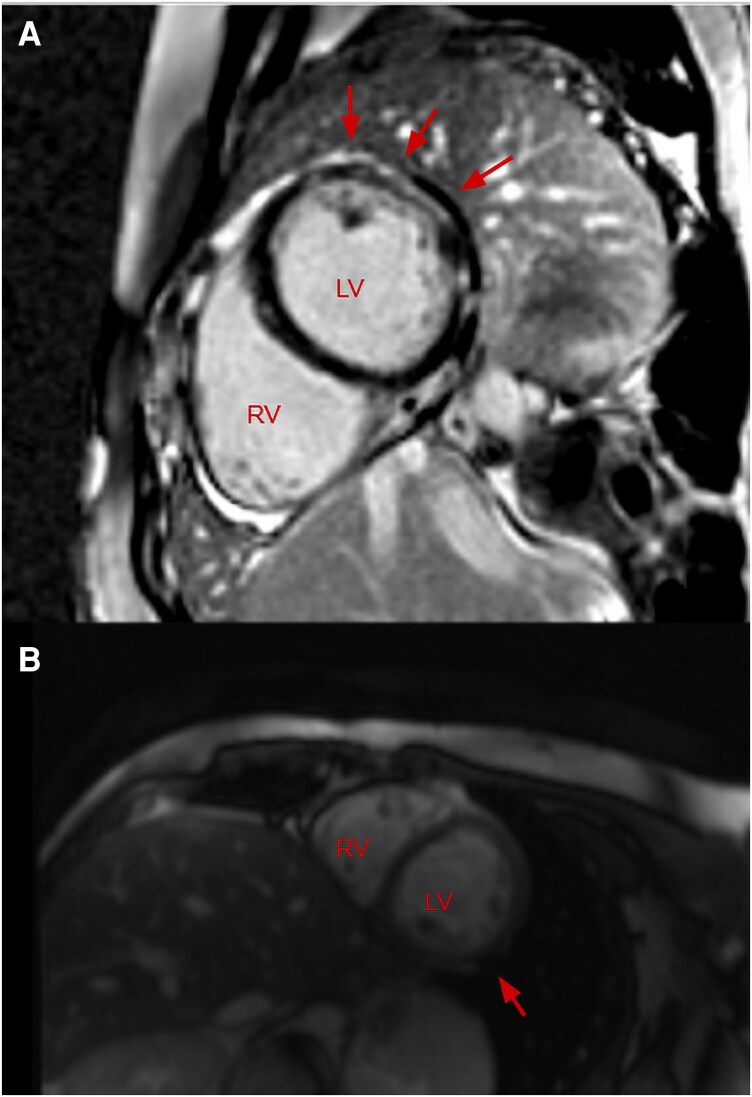
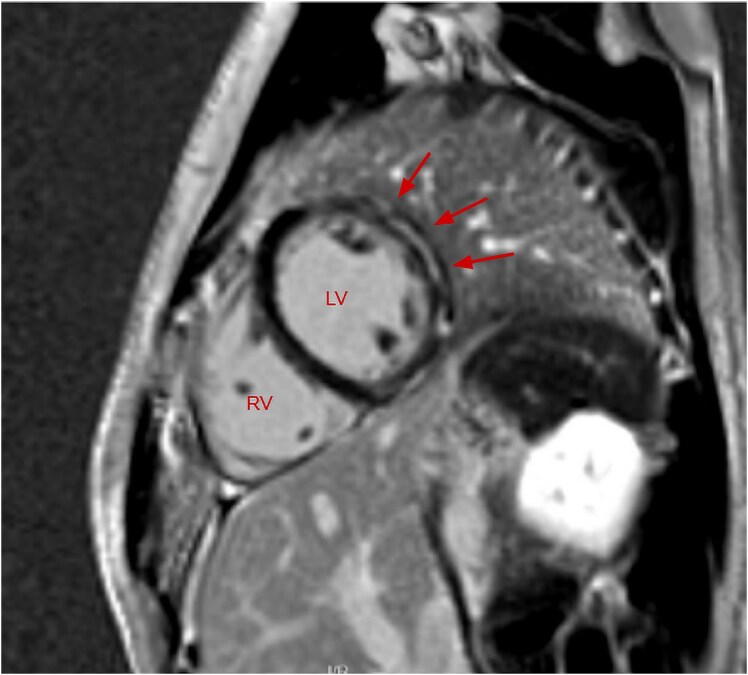
Case summary: A 17-year-old gentleman with a background history of developmental delay, gastrointestinal motility issues, retractile testes, and patellar dislocation presented to our emergency department with chest pain. Investigations revealed static mildly elevated troponin T. An electrocardiogram and transthoracic echocardiogram were both unremarkable. CMR revealed sub-endocardial and mid-wall LGE. He was treated as myocarditis with steroids and colchicine, however symptoms persisted and repeat CMR reported progressive LGE. The diagnosis of myocarditis was reconsidered given an atypical presentation and taking into account his past medical history, and so a whole gene exome was performed. This revealed a dual diagnosis of Klinefelter's Syndrome and a mutation in the dystrophin gene located on the X chromosome.
Discussion: In this case, an interplay between Klinefelter's Syndrome and Muscular Dystrophy is demonstrated, potentially protecting our patient against a more aggressive Duchenne phenotype of muscular dystrophy. Upon non-resolution of symptoms, re-evaluating his presentation, investigations and taking into account his background multi-system medical history lead us to performing the genetic testing which revealed the correct diagnosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


