Domenico Sfondrini, Stefano Marelli, Dario De Martis, Andrea Scribante, Giada Beltramini, Luca Autelitano, Lorenzo Preda
{"title":"单侧双颧植入后眼眶细胞炎及颧周皮瘘:病例报告及文献回顾。","authors":"Domenico Sfondrini, Stefano Marelli, Dario De Martis, Andrea Scribante, Giada Beltramini, Luca Autelitano, Lorenzo Preda","doi":"10.3390/dj13080381","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of zygomatic implants (ZIs) provides a highly predictable treatment option for rehabilitation in patients with severe atrophic maxillae. However, these long implants can potentially cause a number of more serious complications than those seen with conventional dental implants. The aim of this study is to report a case of peri-zygomatic cutaneous fistula following placement of monolateral double zygomatic implants and to analyse the available literature on this complication.</p><p><strong>Methods: </strong>The 55-year-old patient was treated with placement of 3 ZIs, two on the left side. Left periorbital swelling with pain appeared 10 days after surgery with progressive worsening of symptoms. After antibiotic treatment, she developed a left cutaneous fistula with purulent discharge. CT showed two ZIs on the left side with the apical portions in close contact with a 1 cm-wide portion of resorbed zygomatic external cortex and a layer of granulation tissue.</p><p><strong>Results: </strong>Due to the limited amount of bone involved by the fixation tip, the left ZIs were removed and the skin fistula repaired. The patient healed without complications but required prosthesis replacement.</p><p><strong>Conclusions: </strong>After conducting a literature review, peri-zygomatic fistulas seem to be more common in patients with two ZIs placed on the same zygoma. In this case, the amount of available zygomatic bone is relatively limited; the bone drill holes can often be too close together and cause overheating, leading to inter-implant bone resorption and infection, with further orbito-zygomatic fistula development. The authors identified the lack of distance between ZI fixtures as one of the main causes of extraoral ZI infection.</p>","PeriodicalId":11269,"journal":{"name":"Dentistry Journal","volume":"13 8","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385572/pdf/","citationCount":"0","resultStr":"{\"title\":\"Orbital Cellutitis and Peri-Zygomatic Cutaneous Fistula After Monolateral Double Zygomatic Implant Placement: Case Report and Narrative Literature Review.\",\"authors\":\"Domenico Sfondrini, Stefano Marelli, Dario De Martis, Andrea Scribante, Giada Beltramini, Luca Autelitano, Lorenzo Preda\",\"doi\":\"10.3390/dj13080381\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The use of zygomatic implants (ZIs) provides a highly predictable treatment option for rehabilitation in patients with severe atrophic maxillae. However, these long implants can potentially cause a number of more serious complications than those seen with conventional dental implants. The aim of this study is to report a case of peri-zygomatic cutaneous fistula following placement of monolateral double zygomatic implants and to analyse the available literature on this complication.</p><p><strong>Methods: </strong>The 55-year-old patient was treated with placement of 3 ZIs, two on the left side. Left periorbital swelling with pain appeared 10 days after surgery with progressive worsening of symptoms. After antibiotic treatment, she developed a left cutaneous fistula with purulent discharge. CT showed two ZIs on the left side with the apical portions in close contact with a 1 cm-wide portion of resorbed zygomatic external cortex and a layer of granulation tissue.</p><p><strong>Results: </strong>Due to the limited amount of bone involved by the fixation tip, the left ZIs were removed and the skin fistula repaired. The patient healed without complications but required prosthesis replacement.</p><p><strong>Conclusions: </strong>After conducting a literature review, peri-zygomatic fistulas seem to be more common in patients with two ZIs placed on the same zygoma. In this case, the amount of available zygomatic bone is relatively limited; the bone drill holes can often be too close together and cause overheating, leading to inter-implant bone resorption and infection, with further orbito-zygomatic fistula development. The authors identified the lack of distance between ZI fixtures as one of the main causes of extraoral ZI infection.</p>\",\"PeriodicalId\":11269,\"journal\":{\"name\":\"Dentistry Journal\",\"volume\":\"13 8\",\"pages\":\"\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385572/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Dentistry Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/dj13080381\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dentistry Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/dj13080381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
Orbital Cellutitis and Peri-Zygomatic Cutaneous Fistula After Monolateral Double Zygomatic Implant Placement: Case Report and Narrative Literature Review.
Background: The use of zygomatic implants (ZIs) provides a highly predictable treatment option for rehabilitation in patients with severe atrophic maxillae. However, these long implants can potentially cause a number of more serious complications than those seen with conventional dental implants. The aim of this study is to report a case of peri-zygomatic cutaneous fistula following placement of monolateral double zygomatic implants and to analyse the available literature on this complication.
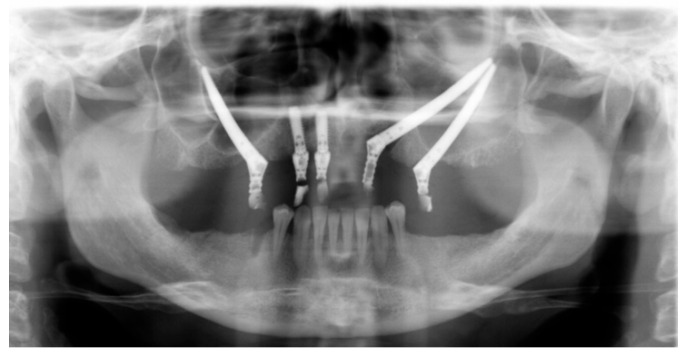
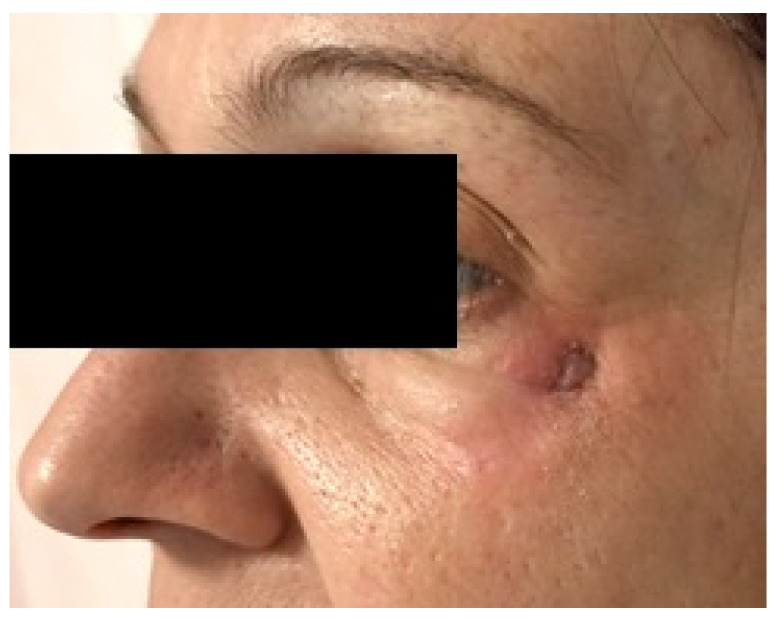
Methods: The 55-year-old patient was treated with placement of 3 ZIs, two on the left side. Left periorbital swelling with pain appeared 10 days after surgery with progressive worsening of symptoms. After antibiotic treatment, she developed a left cutaneous fistula with purulent discharge. CT showed two ZIs on the left side with the apical portions in close contact with a 1 cm-wide portion of resorbed zygomatic external cortex and a layer of granulation tissue.
Results: Due to the limited amount of bone involved by the fixation tip, the left ZIs were removed and the skin fistula repaired. The patient healed without complications but required prosthesis replacement.
Conclusions: After conducting a literature review, peri-zygomatic fistulas seem to be more common in patients with two ZIs placed on the same zygoma. In this case, the amount of available zygomatic bone is relatively limited; the bone drill holes can often be too close together and cause overheating, leading to inter-implant bone resorption and infection, with further orbito-zygomatic fistula development. The authors identified the lack of distance between ZI fixtures as one of the main causes of extraoral ZI infection.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


