{"title":"甲氨蝶呤诱发白细胞破裂性血管炎1例并文献复习。","authors":"Yanisa Ratanapokasatit, Natthachat Jurairattanaporn","doi":"10.2147/CCID.S528734","DOIUrl":null,"url":null,"abstract":"<p><p>Methotrexate (MTX) is widely utilized for the management of autoimmune diseases and neoplasms. It may cause several adverse effects, including myelosuppression, hepatitis, and mucositis, and in rare cases, can result in cutaneous vasculitis. We present a case involving a 60-year-old female patient receiving 5 milligrams (mg) of MTX weekly for the treatment of systemic lupus erythematosus (SLE). Her underlying condition was end-stage renal disease (ESRD), requiring hemodialysis (HD). Ten weeks after MTX treatment, she developed oral ulcers, pancytopenia, and hepatitis, followed by multiple non-blanchable erythematous papules, along with a few vesicles and pustules on the neck, trunk and arms. Laboratory results indicated elevated serum MTX levels, and skin biopsy demonstrated dense superficial perivascular and interstitial lymphocytic, eosinophilic, and neutrophilic infiltration, along with nuclear debris and extravasated erythrocytes, indicative of early leukocytoclastic vasculitis (LCV). Direct immunofluorescence (DIF) identified C3 deposits at the dermo-epidermal junction and superficial blood vessels, indicating possible immune complex-mediated vascular disease. The patient was diagnosed with MTX toxicity and histologically confirmed LCV secondary to MTX. MTX toxicity was effectively treated with intravenous folinic acid and cessation of MTX, alongside prescriptions of oral prednisolone and emollients for LCV management. Serum MTX levels became undetectable after a five-day treatment regimen. Skin lesion resolution occurred within one week. Additionally, a review of existing literatures on MTX-induced LCV was conducted.</p>","PeriodicalId":10447,"journal":{"name":"Clinical, Cosmetic and Investigational Dermatology","volume":"18 ","pages":"2005-2012"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393089/pdf/","citationCount":"0","resultStr":"{\"title\":\"Methotrexate-Induced Leukocytoclastic Vasculitis: A Case Report and Literature Review.\",\"authors\":\"Yanisa Ratanapokasatit, Natthachat Jurairattanaporn\",\"doi\":\"10.2147/CCID.S528734\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Methotrexate (MTX) is widely utilized for the management of autoimmune diseases and neoplasms. It may cause several adverse effects, including myelosuppression, hepatitis, and mucositis, and in rare cases, can result in cutaneous vasculitis. We present a case involving a 60-year-old female patient receiving 5 milligrams (mg) of MTX weekly for the treatment of systemic lupus erythematosus (SLE). Her underlying condition was end-stage renal disease (ESRD), requiring hemodialysis (HD). Ten weeks after MTX treatment, she developed oral ulcers, pancytopenia, and hepatitis, followed by multiple non-blanchable erythematous papules, along with a few vesicles and pustules on the neck, trunk and arms. Laboratory results indicated elevated serum MTX levels, and skin biopsy demonstrated dense superficial perivascular and interstitial lymphocytic, eosinophilic, and neutrophilic infiltration, along with nuclear debris and extravasated erythrocytes, indicative of early leukocytoclastic vasculitis (LCV). Direct immunofluorescence (DIF) identified C3 deposits at the dermo-epidermal junction and superficial blood vessels, indicating possible immune complex-mediated vascular disease. The patient was diagnosed with MTX toxicity and histologically confirmed LCV secondary to MTX. MTX toxicity was effectively treated with intravenous folinic acid and cessation of MTX, alongside prescriptions of oral prednisolone and emollients for LCV management. Serum MTX levels became undetectable after a five-day treatment regimen. Skin lesion resolution occurred within one week. Additionally, a review of existing literatures on MTX-induced LCV was conducted.</p>\",\"PeriodicalId\":10447,\"journal\":{\"name\":\"Clinical, Cosmetic and Investigational Dermatology\",\"volume\":\"18 \",\"pages\":\"2005-2012\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393089/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical, Cosmetic and Investigational Dermatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CCID.S528734\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical, Cosmetic and Investigational Dermatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CCID.S528734","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Methotrexate-Induced Leukocytoclastic Vasculitis: A Case Report and Literature Review.
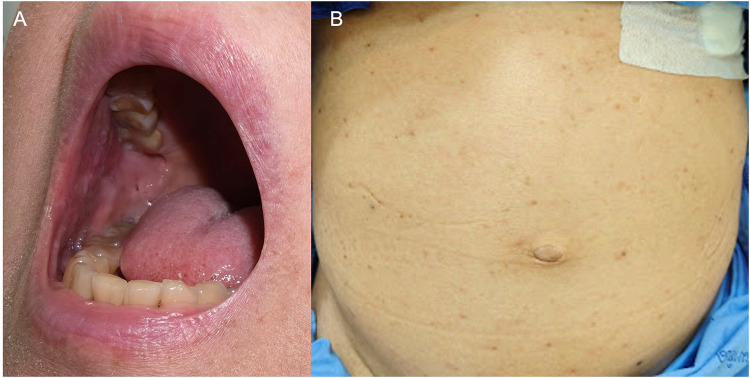
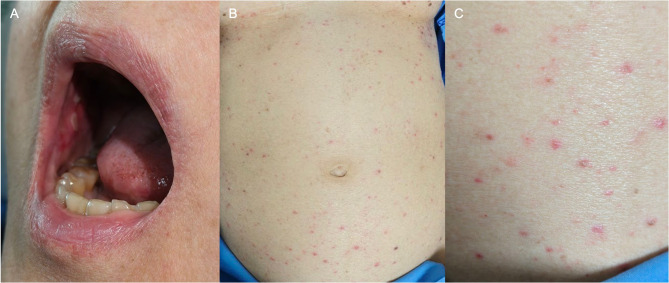
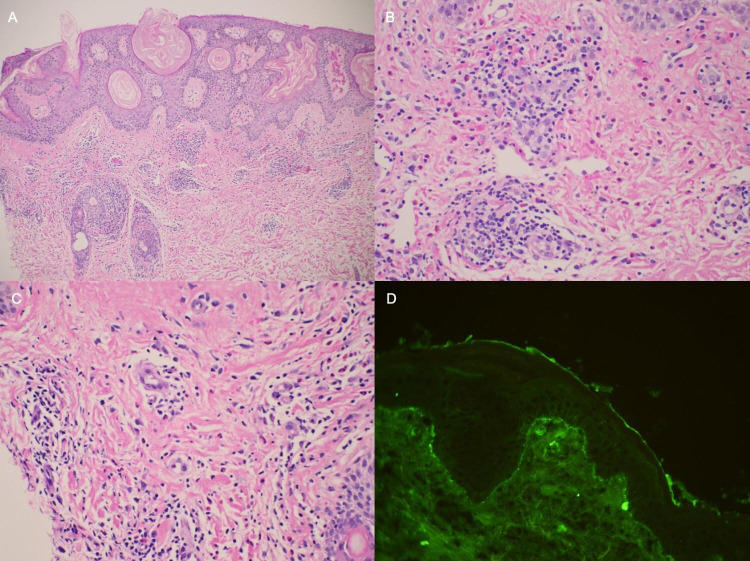
Methotrexate (MTX) is widely utilized for the management of autoimmune diseases and neoplasms. It may cause several adverse effects, including myelosuppression, hepatitis, and mucositis, and in rare cases, can result in cutaneous vasculitis. We present a case involving a 60-year-old female patient receiving 5 milligrams (mg) of MTX weekly for the treatment of systemic lupus erythematosus (SLE). Her underlying condition was end-stage renal disease (ESRD), requiring hemodialysis (HD). Ten weeks after MTX treatment, she developed oral ulcers, pancytopenia, and hepatitis, followed by multiple non-blanchable erythematous papules, along with a few vesicles and pustules on the neck, trunk and arms. Laboratory results indicated elevated serum MTX levels, and skin biopsy demonstrated dense superficial perivascular and interstitial lymphocytic, eosinophilic, and neutrophilic infiltration, along with nuclear debris and extravasated erythrocytes, indicative of early leukocytoclastic vasculitis (LCV). Direct immunofluorescence (DIF) identified C3 deposits at the dermo-epidermal junction and superficial blood vessels, indicating possible immune complex-mediated vascular disease. The patient was diagnosed with MTX toxicity and histologically confirmed LCV secondary to MTX. MTX toxicity was effectively treated with intravenous folinic acid and cessation of MTX, alongside prescriptions of oral prednisolone and emollients for LCV management. Serum MTX levels became undetectable after a five-day treatment regimen. Skin lesion resolution occurred within one week. Additionally, a review of existing literatures on MTX-induced LCV was conducted.
期刊介绍:
Clinical, Cosmetic and Investigational Dermatology is an international, peer-reviewed, open access journal that focuses on the latest clinical and experimental research in all aspects of skin disease and cosmetic interventions. Normal and pathological processes in skin development and aging, their modification and treatment, as well as basic research into histology of dermal and dermal structures that provide clinical insights and potential treatment options are key topics for the journal.
Patient satisfaction, preference, quality of life, compliance, persistence and their role in developing new management options to optimize outcomes for target conditions constitute major areas of interest.
The journal is characterized by the rapid reporting of clinical studies, reviews and original research in skin research and skin care.
All areas of dermatology will be covered; contributions will be welcomed from all clinicians and basic science researchers globally.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


