Ruiji Jiang, Benjamin Beland, Vinil Shah, Min Kang, Douglas B Pet
{"title":"成人肠毒血症肉毒中毒的马尾神经根增强。","authors":"Ruiji Jiang, Benjamin Beland, Vinil Shah, Min Kang, Douglas B Pet","doi":"10.1186/s12883-025-04365-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adult botulism is a rare, life-threatening condition typically caused by exposure to preformed botulinum neurotoxin (BoNT). Acute intestinal toxemia botulism (AITB) is an uncommon subtype resulting from colonization of Clostridium botulinum in the intestines. Diagnosis is made by detecting BoNT in the patient's blood, stool, or gastric fluid. AITB is confirmed when C. botulinum is isolated in culture. Electrodiagnostic studies may support the diagnosis, while imaging-when performed-is generally used to exclude alternative conditions.</p><p><strong>Case presentation: </strong>A 74-year-old man presented with acute dysarthria and ophthalmoparesis, which rapidly progressed to quadriparesis and respiratory failure requiring intubation. Magnetic resonance imaging (MRI) revealed thickening and enhancement of the cauda equina nerve roots. Due to high clinical suspicion for botulism, heptavalent botulinum antitoxin was administered. Intravenous immunoglobulin was also given, as the imaging findings raised concern for an alternative diagnosis of Guillain-Barré syndrome (GBS). Blood and stool samples later tested positive for BoNT type A, and C. botulinum was isolated from the stool, confirming AITB. The patient experienced a gradual but prolonged recovery of motor function following treatment.</p><p><strong>Conclusions: </strong>Botulism in both infants and adults is not typically associated with abnormal neuroimaging findings. To our knowledge, this is the first reported case of cauda equina nerve root thickening and enhancement on MRI in AITB-or in adult botulism more broadly. We outline the differential diagnosis, pathophysiology, and treatment of botulism. This case underscores that abnormal neuroimaging should not delay prompt empiric treatment for botulism when clinical suspicion is high.</p>","PeriodicalId":9170,"journal":{"name":"BMC Neurology","volume":"25 1","pages":"343"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372212/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cauda equina nerve root enhancement in adult intestinal toxemia botulism.\",\"authors\":\"Ruiji Jiang, Benjamin Beland, Vinil Shah, Min Kang, Douglas B Pet\",\"doi\":\"10.1186/s12883-025-04365-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Adult botulism is a rare, life-threatening condition typically caused by exposure to preformed botulinum neurotoxin (BoNT). Acute intestinal toxemia botulism (AITB) is an uncommon subtype resulting from colonization of Clostridium botulinum in the intestines. Diagnosis is made by detecting BoNT in the patient's blood, stool, or gastric fluid. AITB is confirmed when C. botulinum is isolated in culture. Electrodiagnostic studies may support the diagnosis, while imaging-when performed-is generally used to exclude alternative conditions.</p><p><strong>Case presentation: </strong>A 74-year-old man presented with acute dysarthria and ophthalmoparesis, which rapidly progressed to quadriparesis and respiratory failure requiring intubation. Magnetic resonance imaging (MRI) revealed thickening and enhancement of the cauda equina nerve roots. Due to high clinical suspicion for botulism, heptavalent botulinum antitoxin was administered. Intravenous immunoglobulin was also given, as the imaging findings raised concern for an alternative diagnosis of Guillain-Barré syndrome (GBS). Blood and stool samples later tested positive for BoNT type A, and C. botulinum was isolated from the stool, confirming AITB. The patient experienced a gradual but prolonged recovery of motor function following treatment.</p><p><strong>Conclusions: </strong>Botulism in both infants and adults is not typically associated with abnormal neuroimaging findings. To our knowledge, this is the first reported case of cauda equina nerve root thickening and enhancement on MRI in AITB-or in adult botulism more broadly. We outline the differential diagnosis, pathophysiology, and treatment of botulism. This case underscores that abnormal neuroimaging should not delay prompt empiric treatment for botulism when clinical suspicion is high.</p>\",\"PeriodicalId\":9170,\"journal\":{\"name\":\"BMC Neurology\",\"volume\":\"25 1\",\"pages\":\"343\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372212/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12883-025-04365-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12883-025-04365-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Cauda equina nerve root enhancement in adult intestinal toxemia botulism.
Background: Adult botulism is a rare, life-threatening condition typically caused by exposure to preformed botulinum neurotoxin (BoNT). Acute intestinal toxemia botulism (AITB) is an uncommon subtype resulting from colonization of Clostridium botulinum in the intestines. Diagnosis is made by detecting BoNT in the patient's blood, stool, or gastric fluid. AITB is confirmed when C. botulinum is isolated in culture. Electrodiagnostic studies may support the diagnosis, while imaging-when performed-is generally used to exclude alternative conditions.
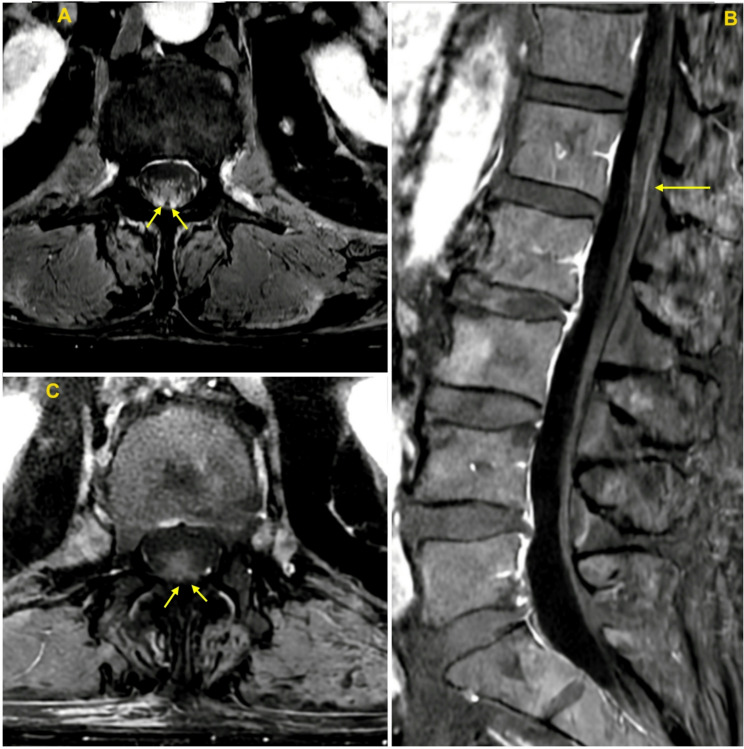
Case presentation: A 74-year-old man presented with acute dysarthria and ophthalmoparesis, which rapidly progressed to quadriparesis and respiratory failure requiring intubation. Magnetic resonance imaging (MRI) revealed thickening and enhancement of the cauda equina nerve roots. Due to high clinical suspicion for botulism, heptavalent botulinum antitoxin was administered. Intravenous immunoglobulin was also given, as the imaging findings raised concern for an alternative diagnosis of Guillain-Barré syndrome (GBS). Blood and stool samples later tested positive for BoNT type A, and C. botulinum was isolated from the stool, confirming AITB. The patient experienced a gradual but prolonged recovery of motor function following treatment.
Conclusions: Botulism in both infants and adults is not typically associated with abnormal neuroimaging findings. To our knowledge, this is the first reported case of cauda equina nerve root thickening and enhancement on MRI in AITB-or in adult botulism more broadly. We outline the differential diagnosis, pathophysiology, and treatment of botulism. This case underscores that abnormal neuroimaging should not delay prompt empiric treatment for botulism when clinical suspicion is high.
期刊介绍:
BMC Neurology is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of neurological disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


