{"title":"开发和评估深度学习模型,用于使用自动目标检测模型检测和分类全视野肢体x线片中的各种骨肿瘤。","authors":"Masashi Yamana, Ryoma Bise, Makoto Endo, Tomoya Matsunobu, Nokitaka Setsu, Nobuhiko Yokoyama, Yasuharu Nakashima, Seiichi Uchida","doi":"10.1302/2046-3758.149.BJR-2024-0505.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>We aim to develop a fully automated deep-learning model to detect and classify benign/malignant bone tumours in full-field limb radiographs using an object detection model. The secondary aim is to identify differences in classification characteristics between the developed automated model, three orthopaedic oncologists, and three general orthopaedic surgeons.</p><p><strong>Methods: </strong>This retrospective analysis included 642 limb bone tumours with 40 diagnoses confirmed pathologically from three institutions (378 benign, 264 malignant including intermediate types). We employed end-to-end object Detection with transformers with Improved deNoising anchOr boxes (DINO) and You Only Look Once (YOLO) models. We performed five-fold cross validation on the collected radiographs, using the training data to train the models, validation data to optimize the models' parameters, and independent test data for final performance evaluation. Firstly, we confirmed DINO achieves a higher detection rate than YOLO. Secondly, we compared the classification performance of DINO with those of doctors, using various metrics such as accuracy, sensitivity, specificity, precision, and F-measure.</p><p><strong>Results: </strong>The DINO model achieved a higher mean tumour detection rate (85.7% (95% CI 81.5 to 89.8)) than the YOLO model (80.1% (95% CI 77.2 to 82.9)). For the evaluation of classification performance, we used 113 cases that DINO detected out of 128 randomly selected cases as the evaluation test set. The accuracy and sensitivity of the DINO model, as a superior model, were significantly higher than those of general orthopaedic surgeons. The DINO model correctly classified 78.6% (22 out of 28 cases) of the challenging cases that two or more doctors misclassified. However, DINO's diagnostic errors primarily occurred with tumours that were diagnostically challenging for orthopaedic oncologists or present in unusual sites.</p><p><strong>Conclusion: </strong>The DINO model automatically detects bone tumours better than the YOLO model, and may assist doctors in detecting tumours and classifying malignant/benign bone tumours in clinical practice.</p>","PeriodicalId":9074,"journal":{"name":"Bone & Joint Research","volume":"14 9","pages":"760-768"},"PeriodicalIF":5.1000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401592/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and evaluation of deep learning models for detecting and classifying various bone tumours in full-field limb radiographs using automated object detection models.\",\"authors\":\"Masashi Yamana, Ryoma Bise, Makoto Endo, Tomoya Matsunobu, Nokitaka Setsu, Nobuhiko Yokoyama, Yasuharu Nakashima, Seiichi Uchida\",\"doi\":\"10.1302/2046-3758.149.BJR-2024-0505.R1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>We aim to develop a fully automated deep-learning model to detect and classify benign/malignant bone tumours in full-field limb radiographs using an object detection model. The secondary aim is to identify differences in classification characteristics between the developed automated model, three orthopaedic oncologists, and three general orthopaedic surgeons.</p><p><strong>Methods: </strong>This retrospective analysis included 642 limb bone tumours with 40 diagnoses confirmed pathologically from three institutions (378 benign, 264 malignant including intermediate types). We employed end-to-end object Detection with transformers with Improved deNoising anchOr boxes (DINO) and You Only Look Once (YOLO) models. We performed five-fold cross validation on the collected radiographs, using the training data to train the models, validation data to optimize the models' parameters, and independent test data for final performance evaluation. Firstly, we confirmed DINO achieves a higher detection rate than YOLO. Secondly, we compared the classification performance of DINO with those of doctors, using various metrics such as accuracy, sensitivity, specificity, precision, and F-measure.</p><p><strong>Results: </strong>The DINO model achieved a higher mean tumour detection rate (85.7% (95% CI 81.5 to 89.8)) than the YOLO model (80.1% (95% CI 77.2 to 82.9)). For the evaluation of classification performance, we used 113 cases that DINO detected out of 128 randomly selected cases as the evaluation test set. The accuracy and sensitivity of the DINO model, as a superior model, were significantly higher than those of general orthopaedic surgeons. The DINO model correctly classified 78.6% (22 out of 28 cases) of the challenging cases that two or more doctors misclassified. However, DINO's diagnostic errors primarily occurred with tumours that were diagnostically challenging for orthopaedic oncologists or present in unusual sites.</p><p><strong>Conclusion: </strong>The DINO model automatically detects bone tumours better than the YOLO model, and may assist doctors in detecting tumours and classifying malignant/benign bone tumours in clinical practice.</p>\",\"PeriodicalId\":9074,\"journal\":{\"name\":\"Bone & Joint Research\",\"volume\":\"14 9\",\"pages\":\"760-768\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2025-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401592/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bone & Joint Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1302/2046-3758.149.BJR-2024-0505.R1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CELL & TISSUE ENGINEERING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1302/2046-3758.149.BJR-2024-0505.R1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL & TISSUE ENGINEERING","Score":null,"Total":0}
引用次数: 0
摘要
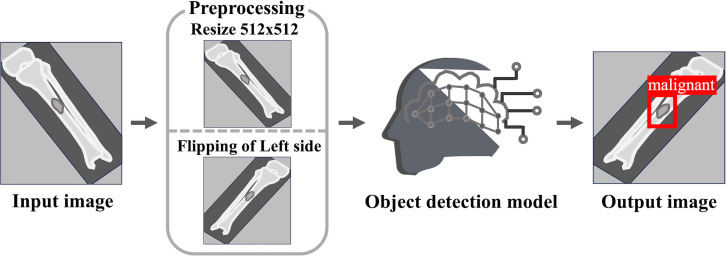
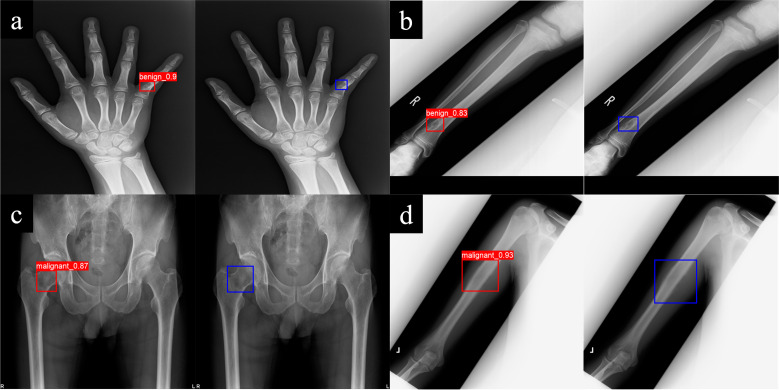
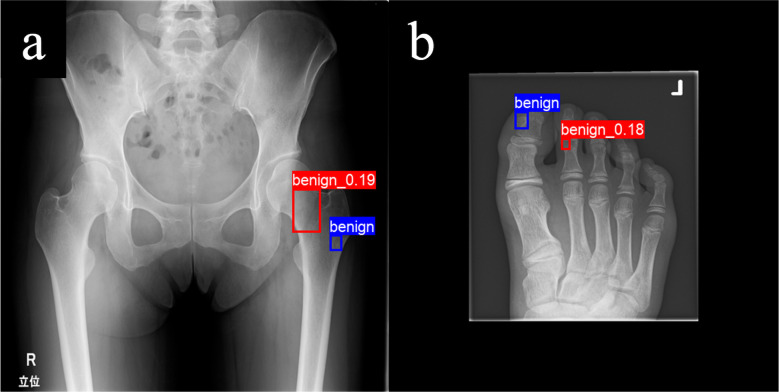
目的:我们的目标是开发一个全自动深度学习模型,使用目标检测模型来检测和分类全视场肢体x线片上的良/恶性骨肿瘤。第二个目的是确定开发的自动化模型、三位骨科肿瘤学家和三位普通骨科医生之间的分类特征差异。方法:回顾性分析3所医院病理确诊的肢体骨肿瘤642例,其中良性378例,恶性264例(含中间型)。我们使用改进的去噪锚盒(DINO)和你只看一次(YOLO)模型的变压器进行端到端目标检测。我们对收集到的x线片进行了五重交叉验证,使用训练数据训练模型,使用验证数据优化模型参数,使用独立测试数据进行最终的性能评估。首先,我们证实DINO比YOLO具有更高的检出率。其次,我们比较了DINO与医生的分类性能,使用各种指标,如准确性、敏感性、特异性、精密度和F-measure。结果:DINO模型的平均肿瘤检出率(85.7% (95% CI 81.5 ~ 89.8))高于YOLO模型(80.1% (95% CI 77.2 ~ 82.9))。为了评价分类性能,我们从128个随机选取的病例中,选取DINO检测到的113例作为评价测试集。DINO模型作为一种优越的模型,其准确性和敏感性均明显高于普通骨科医生的模型。DINO模型正确分类了78.6%(28例中的22例)两个或两个以上医生错误分类的挑战性病例。然而,DINO的诊断错误主要发生在对骨科肿瘤学家来说具有诊断挑战性的肿瘤或出现在不寻常的部位。结论:DINO模型对骨肿瘤的自动检测优于YOLO模型,可在临床中辅助医生对肿瘤的检测和对骨肿瘤的良恶性分类。
Development and evaluation of deep learning models for detecting and classifying various bone tumours in full-field limb radiographs using automated object detection models.
Aims: We aim to develop a fully automated deep-learning model to detect and classify benign/malignant bone tumours in full-field limb radiographs using an object detection model. The secondary aim is to identify differences in classification characteristics between the developed automated model, three orthopaedic oncologists, and three general orthopaedic surgeons.
Methods: This retrospective analysis included 642 limb bone tumours with 40 diagnoses confirmed pathologically from three institutions (378 benign, 264 malignant including intermediate types). We employed end-to-end object Detection with transformers with Improved deNoising anchOr boxes (DINO) and You Only Look Once (YOLO) models. We performed five-fold cross validation on the collected radiographs, using the training data to train the models, validation data to optimize the models' parameters, and independent test data for final performance evaluation. Firstly, we confirmed DINO achieves a higher detection rate than YOLO. Secondly, we compared the classification performance of DINO with those of doctors, using various metrics such as accuracy, sensitivity, specificity, precision, and F-measure.
Results: The DINO model achieved a higher mean tumour detection rate (85.7% (95% CI 81.5 to 89.8)) than the YOLO model (80.1% (95% CI 77.2 to 82.9)). For the evaluation of classification performance, we used 113 cases that DINO detected out of 128 randomly selected cases as the evaluation test set. The accuracy and sensitivity of the DINO model, as a superior model, were significantly higher than those of general orthopaedic surgeons. The DINO model correctly classified 78.6% (22 out of 28 cases) of the challenging cases that two or more doctors misclassified. However, DINO's diagnostic errors primarily occurred with tumours that were diagnostically challenging for orthopaedic oncologists or present in unusual sites.
Conclusion: The DINO model automatically detects bone tumours better than the YOLO model, and may assist doctors in detecting tumours and classifying malignant/benign bone tumours in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


