局部T1定位在心脏结节病诊断和风险分层中的临床应用
IF 2.5
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
摘要
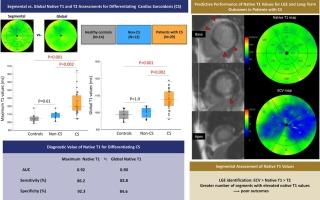
背景心脏结节病(CS)原生T1定位的临床应用和最佳分析方法尚不清楚。本研究探讨节段性原生T1评估在CS患者中的临床价值。方法我们招募了55名参与者,包括41名接受CS诊断评估的患者和14名健康对照。在41例患者中,29例诊断为CS, 12例归类为非CS。使用1.5 t扫描仪评估左心室节段性心脏磁共振结果。主要终点为全因死亡、致死性室性心律失常、心动过缓或因心血管事件住院。结果CS患者的最大T1值和总体T1值显著高于健康对照组和非CS患者。最大T1值和全局T1值在区分CS与其他组方面表现出可比的预测性能,曲线下面积(auc)分别为0.92和0.90。预测晚期钆增强(LGE)节段的AUC以细胞外体积最高,其次是原生T1和T2 (P < 0.05)。具有6个或更多原生T1≥1091 ms的患者预后明显差于无原生T1≥1091 ms的患者(55.6% vs. 18.2%, P = 0.028)。结论最大T1值和全局T1值对CS的鉴别具有较高的预测价值。CS患者的高节段原生T1值可能反映LGE的区域性存在。局部T1评估有助于评估长期预后。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Clinical utility of segmental native T1 mapping for diagnosis and risk-stratification in cardiac sarcoidosis
Background
The clinical utility and optimal analytical approach for native T1 mapping in cardiac sarcoidosis (CS) remain unclear. This study investigated the clinical value of segmental native T1 assessment in patients with CS.
Methods
We recruited 55 participants, including 41 patients undergoing diagnostic evaluation of CS and 14 healthy controls. Of the 41 patients, 29 were diagnosed with CS and 12 were classified as non-CS. Segmental cardiac magnetic resonance findings of the left ventricle were evaluated using a 1.5-T scanner. The primary endpoint was a composite of all-cause death, fatal ventricular arrhythmia, bradycardia, or hospitalization for cardiovascular events.
Results
Maximum and global native T1 values were significantly higher in CS patients than in healthy controls and non-CS patients. Maximum and global T1 values demonstrated comparable predictive performance in differentiating CS from the other groups, with areas under the curve (AUCs) of 0.92 and 0.90, respectively. The AUC for predicting segments with late gadolinium enhancement (LGE) was highest for extracellular volume, followed by native T1 and T2 (P < 0.05 for all). Patients with six or more segments showing native T1 ≥ 1091 ms had a significantly worse prognosis than those without (55.6 % vs. 18.2 %, P = 0.028).
Conclusions
Maximum and global native T1 values were highly predictive for differentiating CS. The high segmental native T1 values in patients with CS may reflect the regional presence of LGE. Segmental native T1 assessment can aid in estimating long-term outcomes.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊
IJC Heart and Vasculature
Medicine-Cardiology and Cardiovascular Medicine
CiteScore
4.90
自引率
10.30%
发文量
216
审稿时长
56 days
期刊介绍:
IJC Heart & Vasculature is an online-only, open-access journal dedicated to publishing original articles and reviews (also Editorials and Letters to the Editor) which report on structural and functional cardiovascular pathology, with an emphasis on imaging and disease pathophysiology. Articles must be authentic, educational, clinically relevant, and original in their content and scientific approach. IJC Heart & Vasculature requires the highest standards of scientific integrity in order to promote reliable, reproducible and verifiable research findings. All authors are advised to consult the Principles of Ethical Publishing in the International Journal of Cardiology before submitting a manuscript. Submission of a manuscript to this journal gives the publisher the right to publish that paper if it is accepted. Manuscripts may be edited to improve clarity and expression.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


