Elizabeth L M Barr, Federica Barzi, Phillip Mills Kulkalgal, Maria Nickels, Sian Graham, Odette Pearson, Varuni Obeyesekere, Wendy E Hoy, Graham R D Jones, Paul D Lawton, Alex D H Brown, Mark Thomas, Ashim Sinha, Alan Cass, Richard J MacIsaac, Louise J Maple-Brown, Jaquelyne T Hughes Wagadagam
{"title":"心脏代谢生物标志物和肾脏疾病进展的预测:eGFR队列研究。","authors":"Elizabeth L M Barr, Federica Barzi, Phillip Mills Kulkalgal, Maria Nickels, Sian Graham, Odette Pearson, Varuni Obeyesekere, Wendy E Hoy, Graham R D Jones, Paul D Lawton, Alex D H Brown, Mark Thomas, Ashim Sinha, Alan Cass, Richard J MacIsaac, Louise J Maple-Brown, Jaquelyne T Hughes Wagadagam","doi":"10.1177/20543581251363126","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditional markers modestly predict chronic kidney disease progression in Aboriginal and Torres Strait Islander people. Therefore, we assessed associations of cardiometabolic and inflammatory clinical biomarkers with kidney disease progression among Aboriginal and Torres Strait Islander people with and without diabetes.</p><p><strong>Objectives: </strong>To identify cardiometabolic and inflammatory clinical biomarkers that predict kidney disease progression in Aboriginal and Torres Strait Islander people.</p><p><strong>Design: </strong>Prospective observational cohort study.</p><p><strong>Setting: </strong>Northern Territory, Australia.</p><p><strong>Participants: </strong>Aboriginal and Torres Strait Islander participants of the estimated glomerular filtration rate (eGFR) study with (n = 218) and without diabetes (n = 278).</p><p><strong>Measurements: </strong>Baseline biomarkers (expressed as 1 standard deviation increase in logarithmic scale), plasma kidney injury molecule-1 (pKIM-1) (pg/ml), high-sensitivity troponin-T (hs-TnT) (ng/L), troponin-I (hs-TnI) (ng/L), and soluble tumor necrosis factor receptor-1 (sTNFR-1) (pg/ml) were assessed in 496 adults. Annual change in eGFR (ml/min/1.73 m<sup>2</sup>) and a composite kidney outcome (first of ≥30% eGFR decline with follow-up eGFR <60 ml/min/1.73 m<sup>2</sup>, initiation of kidney replacement therapy or kidney disease-related death) over a median of 3 years.</p><p><strong>Methods: </strong>Linear regression estimated annual change in eGFR (ml/min/1.73 m<sup>2</sup>). Cox proportional hazards regression estimated hazard ratio (HR) and 95% CI for developing a combined kidney health outcome.</p><p><strong>Results: </strong>In individuals with diabetes, but not those without diabetes, higher baseline hs-TnT (-2.1 [-4.1 to -0.2], <i>P</i> = .033) and sTNFR-1 (-1.8 [-3.5 to -0.1], <i>P</i> = .039) predicted mean (95% CI) eGFR change, after adjusting for age, gender, baseline eGFR, and urinary albumin-to-creatinine ratio. Baseline variables explained 11% of eGFR decline variance; increasing to 27% (<i>P</i> < .001) with biomarkers. In diabetes, hs-TnT and hs-TnI were significantly associated with increased risk of kidney health outcomes.</p><p><strong>Limitations: </strong>Limitations included potential chronic kidney disease misclassification from single creatinine and albumin measurements, limited adjustment for covariates due to a small sample size, and short follow-up restricting long-term outcome assessment.</p><p><strong>Conclusions: </strong>Cardiovascular, kidney, and inflammatory biomarkers are likely associated with kidney function loss in diabetes, with particularly prominent associations for cardiac injury markers.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251363126"},"PeriodicalIF":1.5000,"publicationDate":"2025-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12358709/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiometabolic Biomarkers and Prediction of Kidney Disease Progression: The eGFR Cohort Study.\",\"authors\":\"Elizabeth L M Barr, Federica Barzi, Phillip Mills Kulkalgal, Maria Nickels, Sian Graham, Odette Pearson, Varuni Obeyesekere, Wendy E Hoy, Graham R D Jones, Paul D Lawton, Alex D H Brown, Mark Thomas, Ashim Sinha, Alan Cass, Richard J MacIsaac, Louise J Maple-Brown, Jaquelyne T Hughes Wagadagam\",\"doi\":\"10.1177/20543581251363126\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Traditional markers modestly predict chronic kidney disease progression in Aboriginal and Torres Strait Islander people. Therefore, we assessed associations of cardiometabolic and inflammatory clinical biomarkers with kidney disease progression among Aboriginal and Torres Strait Islander people with and without diabetes.</p><p><strong>Objectives: </strong>To identify cardiometabolic and inflammatory clinical biomarkers that predict kidney disease progression in Aboriginal and Torres Strait Islander people.</p><p><strong>Design: </strong>Prospective observational cohort study.</p><p><strong>Setting: </strong>Northern Territory, Australia.</p><p><strong>Participants: </strong>Aboriginal and Torres Strait Islander participants of the estimated glomerular filtration rate (eGFR) study with (n = 218) and without diabetes (n = 278).</p><p><strong>Measurements: </strong>Baseline biomarkers (expressed as 1 standard deviation increase in logarithmic scale), plasma kidney injury molecule-1 (pKIM-1) (pg/ml), high-sensitivity troponin-T (hs-TnT) (ng/L), troponin-I (hs-TnI) (ng/L), and soluble tumor necrosis factor receptor-1 (sTNFR-1) (pg/ml) were assessed in 496 adults. Annual change in eGFR (ml/min/1.73 m<sup>2</sup>) and a composite kidney outcome (first of ≥30% eGFR decline with follow-up eGFR <60 ml/min/1.73 m<sup>2</sup>, initiation of kidney replacement therapy or kidney disease-related death) over a median of 3 years.</p><p><strong>Methods: </strong>Linear regression estimated annual change in eGFR (ml/min/1.73 m<sup>2</sup>). Cox proportional hazards regression estimated hazard ratio (HR) and 95% CI for developing a combined kidney health outcome.</p><p><strong>Results: </strong>In individuals with diabetes, but not those without diabetes, higher baseline hs-TnT (-2.1 [-4.1 to -0.2], <i>P</i> = .033) and sTNFR-1 (-1.8 [-3.5 to -0.1], <i>P</i> = .039) predicted mean (95% CI) eGFR change, after adjusting for age, gender, baseline eGFR, and urinary albumin-to-creatinine ratio. Baseline variables explained 11% of eGFR decline variance; increasing to 27% (<i>P</i> < .001) with biomarkers. In diabetes, hs-TnT and hs-TnI were significantly associated with increased risk of kidney health outcomes.</p><p><strong>Limitations: </strong>Limitations included potential chronic kidney disease misclassification from single creatinine and albumin measurements, limited adjustment for covariates due to a small sample size, and short follow-up restricting long-term outcome assessment.</p><p><strong>Conclusions: </strong>Cardiovascular, kidney, and inflammatory biomarkers are likely associated with kidney function loss in diabetes, with particularly prominent associations for cardiac injury markers.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581251363126\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-08-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12358709/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581251363126\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251363126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Cardiometabolic Biomarkers and Prediction of Kidney Disease Progression: The eGFR Cohort Study.
Background: Traditional markers modestly predict chronic kidney disease progression in Aboriginal and Torres Strait Islander people. Therefore, we assessed associations of cardiometabolic and inflammatory clinical biomarkers with kidney disease progression among Aboriginal and Torres Strait Islander people with and without diabetes.
Objectives: To identify cardiometabolic and inflammatory clinical biomarkers that predict kidney disease progression in Aboriginal and Torres Strait Islander people.
Design: Prospective observational cohort study.
Setting: Northern Territory, Australia.
Participants: Aboriginal and Torres Strait Islander participants of the estimated glomerular filtration rate (eGFR) study with (n = 218) and without diabetes (n = 278).
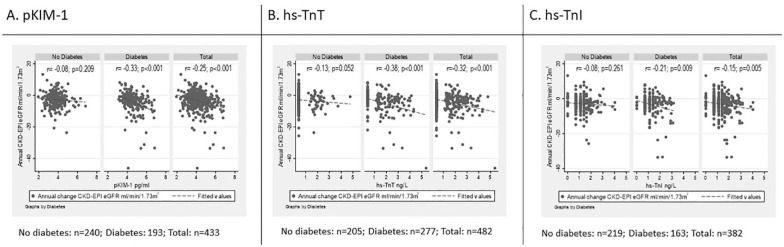
Measurements: Baseline biomarkers (expressed as 1 standard deviation increase in logarithmic scale), plasma kidney injury molecule-1 (pKIM-1) (pg/ml), high-sensitivity troponin-T (hs-TnT) (ng/L), troponin-I (hs-TnI) (ng/L), and soluble tumor necrosis factor receptor-1 (sTNFR-1) (pg/ml) were assessed in 496 adults. Annual change in eGFR (ml/min/1.73 m2) and a composite kidney outcome (first of ≥30% eGFR decline with follow-up eGFR <60 ml/min/1.73 m2, initiation of kidney replacement therapy or kidney disease-related death) over a median of 3 years.
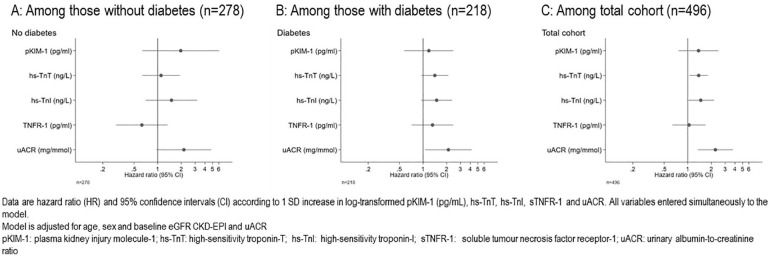
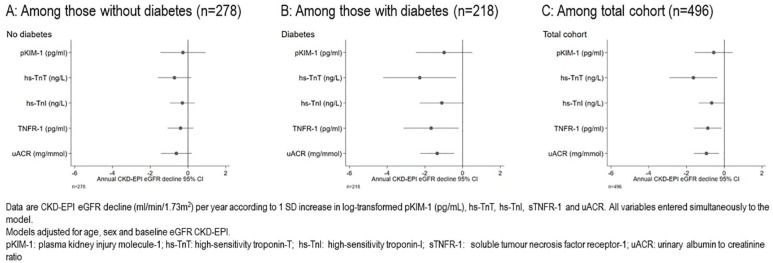
Methods: Linear regression estimated annual change in eGFR (ml/min/1.73 m2). Cox proportional hazards regression estimated hazard ratio (HR) and 95% CI for developing a combined kidney health outcome.
Results: In individuals with diabetes, but not those without diabetes, higher baseline hs-TnT (-2.1 [-4.1 to -0.2], P = .033) and sTNFR-1 (-1.8 [-3.5 to -0.1], P = .039) predicted mean (95% CI) eGFR change, after adjusting for age, gender, baseline eGFR, and urinary albumin-to-creatinine ratio. Baseline variables explained 11% of eGFR decline variance; increasing to 27% (P < .001) with biomarkers. In diabetes, hs-TnT and hs-TnI were significantly associated with increased risk of kidney health outcomes.
Limitations: Limitations included potential chronic kidney disease misclassification from single creatinine and albumin measurements, limited adjustment for covariates due to a small sample size, and short follow-up restricting long-term outcome assessment.
Conclusions: Cardiovascular, kidney, and inflammatory biomarkers are likely associated with kidney function loss in diabetes, with particularly prominent associations for cardiac injury markers.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


