{"title":"妊娠期尿崩症合并库欣综合征1例。","authors":"Shinnosuke Hata, Nobuyoshi Shinokawa, Yuki Harada, Chisato Kato, Saki Ota, Osamu Takaoka, Tsukasa Narukawa, Hiroya Iwase, Toru Tanaka","doi":"10.1186/s12902-025-01946-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cushing's syndrome (CS) during pregnancy is a rare condition associated with significant maternal and fetal complications, including hypertension, diabetes, preeclampsia, and preterm birth. Diabetes insipidus (DI) in pregnancy is a rare but often diagnosed condition, and its effective management is crucial for maintaining maternal health during pregnancy and childbirth. This case report describes the rare coexistence of DI and CS during pregnancy, highlighting the unique complexities in diagnosis and management.</p><p><strong>Case presentation: </strong>A 29-year-old woman with a history of pregnancy-induced hypertension developed severe hypertension, hypokalemia, and polyuria (6.6 L/day) during her 7th pregnancy. Laboratory findings showed elevated cortisol, suppressed adrenocorticotropic hormone (ACTH), and a 30-mm left adrenal mass, confirming adrenal CS. Despite potassium supplementation, persistent polyuria and fluid imbalance necessitated initiating desmopressin therapy at 27 weeks of gestation. The patient subsequently developed preeclampsia and underwent emergency cesarean section at 29 weeks, delivering a 1197-g infant with a very low birth weight. Polyuria resolved postpartum, and she underwent left adrenalectomy after discharge.</p><p><strong>Conclusions: </strong>This case illustrates the complexity of managing coexisting CS and GDI during pregnancy, emphasizing the importance of considering alternative mechanisms, such as cortisol-induced antidiuretic hormone resistance, in polyuria. Multidisciplinary approaches are crucial to optimizing maternal and fetal outcomes in rare endocrine conditions, and help contribute to the understanding of CS and DI interactions during pregnancy.</p>","PeriodicalId":9152,"journal":{"name":"BMC Endocrine Disorders","volume":"25 1","pages":"197"},"PeriodicalIF":3.3000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366015/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cushing's syndrome with diabetes insipidus in pregnancy: a case report.\",\"authors\":\"Shinnosuke Hata, Nobuyoshi Shinokawa, Yuki Harada, Chisato Kato, Saki Ota, Osamu Takaoka, Tsukasa Narukawa, Hiroya Iwase, Toru Tanaka\",\"doi\":\"10.1186/s12902-025-01946-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cushing's syndrome (CS) during pregnancy is a rare condition associated with significant maternal and fetal complications, including hypertension, diabetes, preeclampsia, and preterm birth. Diabetes insipidus (DI) in pregnancy is a rare but often diagnosed condition, and its effective management is crucial for maintaining maternal health during pregnancy and childbirth. This case report describes the rare coexistence of DI and CS during pregnancy, highlighting the unique complexities in diagnosis and management.</p><p><strong>Case presentation: </strong>A 29-year-old woman with a history of pregnancy-induced hypertension developed severe hypertension, hypokalemia, and polyuria (6.6 L/day) during her 7th pregnancy. Laboratory findings showed elevated cortisol, suppressed adrenocorticotropic hormone (ACTH), and a 30-mm left adrenal mass, confirming adrenal CS. Despite potassium supplementation, persistent polyuria and fluid imbalance necessitated initiating desmopressin therapy at 27 weeks of gestation. The patient subsequently developed preeclampsia and underwent emergency cesarean section at 29 weeks, delivering a 1197-g infant with a very low birth weight. Polyuria resolved postpartum, and she underwent left adrenalectomy after discharge.</p><p><strong>Conclusions: </strong>This case illustrates the complexity of managing coexisting CS and GDI during pregnancy, emphasizing the importance of considering alternative mechanisms, such as cortisol-induced antidiuretic hormone resistance, in polyuria. Multidisciplinary approaches are crucial to optimizing maternal and fetal outcomes in rare endocrine conditions, and help contribute to the understanding of CS and DI interactions during pregnancy.</p>\",\"PeriodicalId\":9152,\"journal\":{\"name\":\"BMC Endocrine Disorders\",\"volume\":\"25 1\",\"pages\":\"197\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-08-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366015/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Endocrine Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12902-025-01946-9\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Endocrine Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12902-025-01946-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Cushing's syndrome with diabetes insipidus in pregnancy: a case report.
Background: Cushing's syndrome (CS) during pregnancy is a rare condition associated with significant maternal and fetal complications, including hypertension, diabetes, preeclampsia, and preterm birth. Diabetes insipidus (DI) in pregnancy is a rare but often diagnosed condition, and its effective management is crucial for maintaining maternal health during pregnancy and childbirth. This case report describes the rare coexistence of DI and CS during pregnancy, highlighting the unique complexities in diagnosis and management.
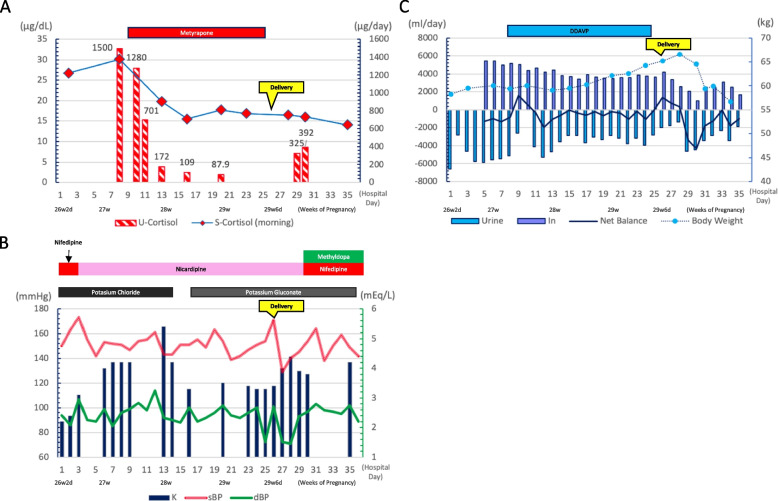
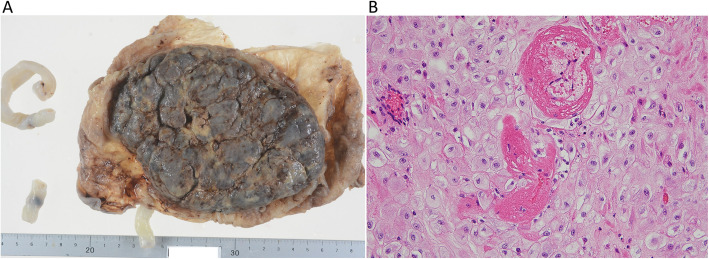
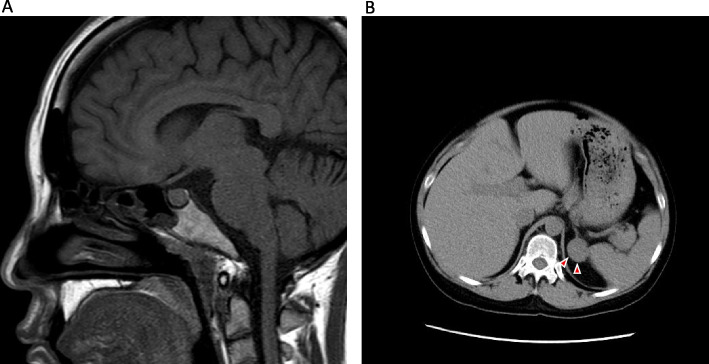
Case presentation: A 29-year-old woman with a history of pregnancy-induced hypertension developed severe hypertension, hypokalemia, and polyuria (6.6 L/day) during her 7th pregnancy. Laboratory findings showed elevated cortisol, suppressed adrenocorticotropic hormone (ACTH), and a 30-mm left adrenal mass, confirming adrenal CS. Despite potassium supplementation, persistent polyuria and fluid imbalance necessitated initiating desmopressin therapy at 27 weeks of gestation. The patient subsequently developed preeclampsia and underwent emergency cesarean section at 29 weeks, delivering a 1197-g infant with a very low birth weight. Polyuria resolved postpartum, and she underwent left adrenalectomy after discharge.
Conclusions: This case illustrates the complexity of managing coexisting CS and GDI during pregnancy, emphasizing the importance of considering alternative mechanisms, such as cortisol-induced antidiuretic hormone resistance, in polyuria. Multidisciplinary approaches are crucial to optimizing maternal and fetal outcomes in rare endocrine conditions, and help contribute to the understanding of CS and DI interactions during pregnancy.
期刊介绍:
BMC Endocrine Disorders is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of endocrine disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


