Yujiao Wang, Ting Mu, Yufen Fu, Yuxin Wang, Guoping Li
{"title":"慢性阻塞性肺疾病稳定和急性加重期的生物年龄建模","authors":"Yujiao Wang, Ting Mu, Yufen Fu, Yuxin Wang, Guoping Li","doi":"10.1186/s12890-025-03841-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aging has been established as an independent risk factor for chronic obstructive pulmonary disease (COPD). Biological age (BA), a novel metric for gauging the extent of aging, has rarely been investigated in the context of acute exacerbation of COPD (AECOPD). Our study aimed to elucidate the association between BA and AECOPD, thereby highlighting the potential of BA as a predictive tool in clinical practice.</p><p><strong>Methods: </strong>The dataset encompasses patients hospitalized at Chengdu Third People's Hospital between 2018 and 2022. The AECOPD patients enrolled in this study were hospitalized due to rapidly worsening symptoms, including cough, sputum production, and dyspnea, whereas the COPD patients were clinically stable. BA and biological age acceleration were ascertained through the Klemera-Doubale method (KDM). A multivariable logistic regression analysis was conducted to evaluate the correlation between BA, biological age acceleration, and the incidence of AECOPD, complemented by subgroup analyses to explore the dose‒response dynamics between biological age acceleration and the risk of AECOPD. The dataset was partitioned into training and validation sets at a 7:3 ratio, and LASSO regression was applied to refine the model's variable composition. To assess the ability of different variables to discriminate current disease status, we developed the initial model and three subsequent models, with the following variables added in the new model: Chronological age (CA), BA, and biological age acceleration. The models were subsequently evaluated within both datasets.</p><p><strong>Results: </strong>The study cohort comprised 2,511 patients, through an analysis of the transect data, with 59.1% experiencing acute exacerbations. Both BA (79.14 ± 9.49 years) and biological age acceleration (1.04 ± 2.82 years) emerged as independent risk factors for AECOPD (P < 0.001). In Model 3, each year increment in BA and biological age acceleration corresponded to a 1.04-fold (95% CI = 1.027-1.048, P < 0.001) and 1.18-fold (95% CI = 1.14-1.224, P < 0.001) increase in exacerbation risk, respectively. The biological age of patients with stable COPD was significantly lower than the actual age (-0.36 ± 2.56 years), which suggests a significant inter-individual heterogeneity in the biological aging process of COPD patients. Subgroup analysis confirmed a pronounced dose‒response relationship between biological age acceleration and AECOPD risk(Q4 vs. Q1: OR = 2.7, 95% CI = 2.172-3.518). LASSO regression pinpointed BMI, Diabetes, Hypertensive heart disease, Cor pulmonale, Stroke, and Hyperlipidemia as critical variables within the model. The internal validation process revealed AUC values of 0.735 (95% CI = 0.7-0.77), 0.742 (95% CI = 0.707-0.777), 0.753 (95% CI = 0.719-0.787), and 0.766 (95% CI = 0.733-0.8) for the respective models. The HL test confirmed the models' good fit (P = 0.128, P = 0.121, P = 0.272, P = 0.795), with Model 4 exhibiting the most precise calibration against the diagonal reference. Decision curve analysis (DCA) indicated that all the models provided a net benefit in disease outcome discrimination, with Model 4 yielding the most significant advantage.</p><p><strong>Conclusions: </strong>The acceleration of aging portends an increased propensity for acute exacerbations, and a distinct dose-response relationship is observable between biological age acceleration and exacerbation events. BA and biological age acceleration outperform chronological age in discerning the likelihood of acute exacerbations, underscoring their enhanced ability to predict this critical health outcome.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"398"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366205/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modelling of biological age in stable and acute exacerbations of chronic obstructive pulmonary disease.\",\"authors\":\"Yujiao Wang, Ting Mu, Yufen Fu, Yuxin Wang, Guoping Li\",\"doi\":\"10.1186/s12890-025-03841-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Aging has been established as an independent risk factor for chronic obstructive pulmonary disease (COPD). Biological age (BA), a novel metric for gauging the extent of aging, has rarely been investigated in the context of acute exacerbation of COPD (AECOPD). Our study aimed to elucidate the association between BA and AECOPD, thereby highlighting the potential of BA as a predictive tool in clinical practice.</p><p><strong>Methods: </strong>The dataset encompasses patients hospitalized at Chengdu Third People's Hospital between 2018 and 2022. The AECOPD patients enrolled in this study were hospitalized due to rapidly worsening symptoms, including cough, sputum production, and dyspnea, whereas the COPD patients were clinically stable. BA and biological age acceleration were ascertained through the Klemera-Doubale method (KDM). A multivariable logistic regression analysis was conducted to evaluate the correlation between BA, biological age acceleration, and the incidence of AECOPD, complemented by subgroup analyses to explore the dose‒response dynamics between biological age acceleration and the risk of AECOPD. The dataset was partitioned into training and validation sets at a 7:3 ratio, and LASSO regression was applied to refine the model's variable composition. To assess the ability of different variables to discriminate current disease status, we developed the initial model and three subsequent models, with the following variables added in the new model: Chronological age (CA), BA, and biological age acceleration. The models were subsequently evaluated within both datasets.</p><p><strong>Results: </strong>The study cohort comprised 2,511 patients, through an analysis of the transect data, with 59.1% experiencing acute exacerbations. Both BA (79.14 ± 9.49 years) and biological age acceleration (1.04 ± 2.82 years) emerged as independent risk factors for AECOPD (P < 0.001). In Model 3, each year increment in BA and biological age acceleration corresponded to a 1.04-fold (95% CI = 1.027-1.048, P < 0.001) and 1.18-fold (95% CI = 1.14-1.224, P < 0.001) increase in exacerbation risk, respectively. The biological age of patients with stable COPD was significantly lower than the actual age (-0.36 ± 2.56 years), which suggests a significant inter-individual heterogeneity in the biological aging process of COPD patients. Subgroup analysis confirmed a pronounced dose‒response relationship between biological age acceleration and AECOPD risk(Q4 vs. Q1: OR = 2.7, 95% CI = 2.172-3.518). LASSO regression pinpointed BMI, Diabetes, Hypertensive heart disease, Cor pulmonale, Stroke, and Hyperlipidemia as critical variables within the model. The internal validation process revealed AUC values of 0.735 (95% CI = 0.7-0.77), 0.742 (95% CI = 0.707-0.777), 0.753 (95% CI = 0.719-0.787), and 0.766 (95% CI = 0.733-0.8) for the respective models. The HL test confirmed the models' good fit (P = 0.128, P = 0.121, P = 0.272, P = 0.795), with Model 4 exhibiting the most precise calibration against the diagonal reference. Decision curve analysis (DCA) indicated that all the models provided a net benefit in disease outcome discrimination, with Model 4 yielding the most significant advantage.</p><p><strong>Conclusions: </strong>The acceleration of aging portends an increased propensity for acute exacerbations, and a distinct dose-response relationship is observable between biological age acceleration and exacerbation events. BA and biological age acceleration outperform chronological age in discerning the likelihood of acute exacerbations, underscoring their enhanced ability to predict this critical health outcome.</p>\",\"PeriodicalId\":9148,\"journal\":{\"name\":\"BMC Pulmonary Medicine\",\"volume\":\"25 1\",\"pages\":\"398\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366205/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pulmonary Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12890-025-03841-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03841-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Modelling of biological age in stable and acute exacerbations of chronic obstructive pulmonary disease.
Background: Aging has been established as an independent risk factor for chronic obstructive pulmonary disease (COPD). Biological age (BA), a novel metric for gauging the extent of aging, has rarely been investigated in the context of acute exacerbation of COPD (AECOPD). Our study aimed to elucidate the association between BA and AECOPD, thereby highlighting the potential of BA as a predictive tool in clinical practice.
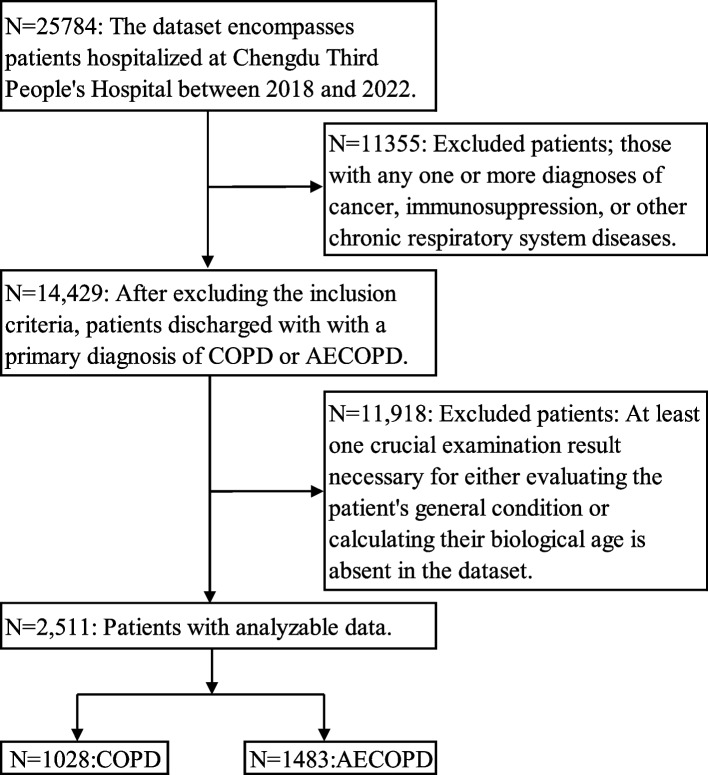
Methods: The dataset encompasses patients hospitalized at Chengdu Third People's Hospital between 2018 and 2022. The AECOPD patients enrolled in this study were hospitalized due to rapidly worsening symptoms, including cough, sputum production, and dyspnea, whereas the COPD patients were clinically stable. BA and biological age acceleration were ascertained through the Klemera-Doubale method (KDM). A multivariable logistic regression analysis was conducted to evaluate the correlation between BA, biological age acceleration, and the incidence of AECOPD, complemented by subgroup analyses to explore the dose‒response dynamics between biological age acceleration and the risk of AECOPD. The dataset was partitioned into training and validation sets at a 7:3 ratio, and LASSO regression was applied to refine the model's variable composition. To assess the ability of different variables to discriminate current disease status, we developed the initial model and three subsequent models, with the following variables added in the new model: Chronological age (CA), BA, and biological age acceleration. The models were subsequently evaluated within both datasets.
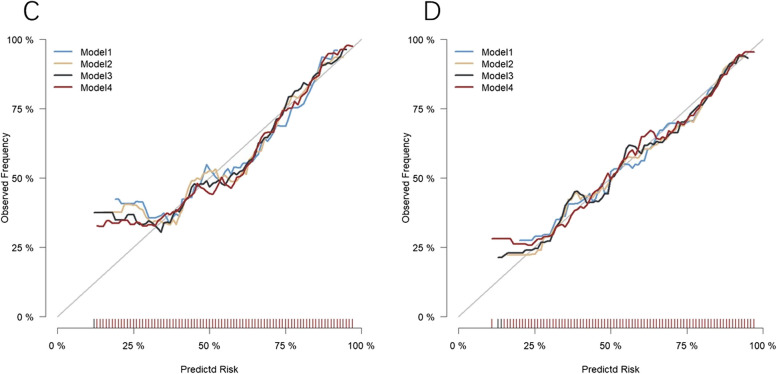
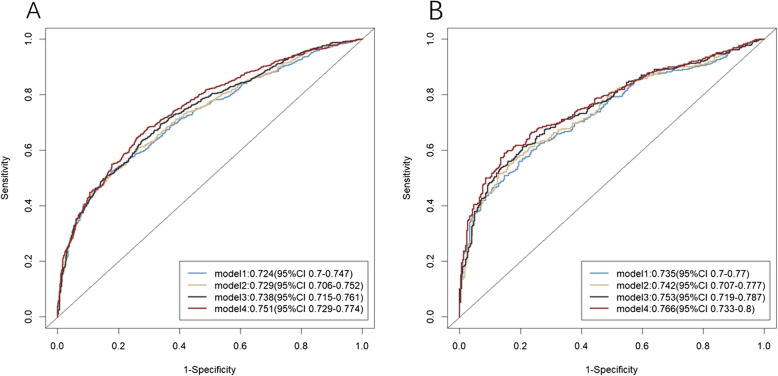
Results: The study cohort comprised 2,511 patients, through an analysis of the transect data, with 59.1% experiencing acute exacerbations. Both BA (79.14 ± 9.49 years) and biological age acceleration (1.04 ± 2.82 years) emerged as independent risk factors for AECOPD (P < 0.001). In Model 3, each year increment in BA and biological age acceleration corresponded to a 1.04-fold (95% CI = 1.027-1.048, P < 0.001) and 1.18-fold (95% CI = 1.14-1.224, P < 0.001) increase in exacerbation risk, respectively. The biological age of patients with stable COPD was significantly lower than the actual age (-0.36 ± 2.56 years), which suggests a significant inter-individual heterogeneity in the biological aging process of COPD patients. Subgroup analysis confirmed a pronounced dose‒response relationship between biological age acceleration and AECOPD risk(Q4 vs. Q1: OR = 2.7, 95% CI = 2.172-3.518). LASSO regression pinpointed BMI, Diabetes, Hypertensive heart disease, Cor pulmonale, Stroke, and Hyperlipidemia as critical variables within the model. The internal validation process revealed AUC values of 0.735 (95% CI = 0.7-0.77), 0.742 (95% CI = 0.707-0.777), 0.753 (95% CI = 0.719-0.787), and 0.766 (95% CI = 0.733-0.8) for the respective models. The HL test confirmed the models' good fit (P = 0.128, P = 0.121, P = 0.272, P = 0.795), with Model 4 exhibiting the most precise calibration against the diagonal reference. Decision curve analysis (DCA) indicated that all the models provided a net benefit in disease outcome discrimination, with Model 4 yielding the most significant advantage.
Conclusions: The acceleration of aging portends an increased propensity for acute exacerbations, and a distinct dose-response relationship is observable between biological age acceleration and exacerbation events. BA and biological age acceleration outperform chronological age in discerning the likelihood of acute exacerbations, underscoring their enhanced ability to predict this critical health outcome.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


