Panagiota Fallon, Melissa Matthews, Abhisekh Chatterjee, Dimitrios Sapountzis, Nikolaos Chatzikrachtis, Katie McComb, Samuel Bishara, Ivo Donkov, Konstantinos Charitopoulos, Panagiotis Nikolinakos
{"title":"输尿管小肠瘘的治疗:1例报告及文献复习。","authors":"Panagiota Fallon, Melissa Matthews, Abhisekh Chatterjee, Dimitrios Sapountzis, Nikolaos Chatzikrachtis, Katie McComb, Samuel Bishara, Ivo Donkov, Konstantinos Charitopoulos, Panagiotis Nikolinakos","doi":"10.1155/criu/7232300","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Ureteric small bowel fistulas are rare entities, with limited reports in the literature. These pathological connections between the ureter and small bowel can lead to recurrent upper urinary tract infections and pose significant diagnostic and therapeutic challenges. The primary cause of ureteric small bowel fistula formation is iatrogenic intervention, such as percutaneous nephrolithotomy (PCNL) or abdominal surgery involving tissue resection. However, they can also arise spontaneously due to local chronic inflammation and infection. Given their rarity, there is no standardised management pathway, and the treatment approach should be individualised. <b>Case Presentation:</b> We present the case of a 57-year-old man presenting with a history of extensive locally advanced distal sigmoid carcinoma, managed with Hartmann's procedure with end colostomy followed by adjuvant radiotherapy and chemotherapy. He later developed a mid-ureteric small bowel fistula, presenting with urosepsis, a high-output stoma, deteriorating renal function and severe metabolic acidosis. Conservative management with regular ureteric stent exchanges every 3-4 months has successfully preserved renal function and improved his quality of life. Surgical closure was not pursued due to high operative risk, and repeat imaging has shown no evidence of persisting fistula, suggesting possible spontaneous closure. <b>Conclusion:</b> The treatment options for this ureteric small bowel fistula were limited. A lifelong nephrostomy was deemed unsuitable due to incompatibility with the patient's profession, and surgical intervention was associated with significant complexity due to the patient's history of malignancy and radiotherapy-related tissue changes. Therefore, a conservative strategy involving serial ureteric stent exchanges was pursued. Early recognition and individualised treatment of ureteric-enteric fistulas are essential, as timely intervention can significantly enhance prognosis and quality of life.</p>","PeriodicalId":30323,"journal":{"name":"Case Reports in Urology","volume":"2025 ","pages":"7232300"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12356682/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of Ureteric Small Bowel Fistula: A Case Report and Review of the Current Literature.\",\"authors\":\"Panagiota Fallon, Melissa Matthews, Abhisekh Chatterjee, Dimitrios Sapountzis, Nikolaos Chatzikrachtis, Katie McComb, Samuel Bishara, Ivo Donkov, Konstantinos Charitopoulos, Panagiotis Nikolinakos\",\"doi\":\"10.1155/criu/7232300\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Ureteric small bowel fistulas are rare entities, with limited reports in the literature. These pathological connections between the ureter and small bowel can lead to recurrent upper urinary tract infections and pose significant diagnostic and therapeutic challenges. The primary cause of ureteric small bowel fistula formation is iatrogenic intervention, such as percutaneous nephrolithotomy (PCNL) or abdominal surgery involving tissue resection. However, they can also arise spontaneously due to local chronic inflammation and infection. Given their rarity, there is no standardised management pathway, and the treatment approach should be individualised. <b>Case Presentation:</b> We present the case of a 57-year-old man presenting with a history of extensive locally advanced distal sigmoid carcinoma, managed with Hartmann's procedure with end colostomy followed by adjuvant radiotherapy and chemotherapy. He later developed a mid-ureteric small bowel fistula, presenting with urosepsis, a high-output stoma, deteriorating renal function and severe metabolic acidosis. Conservative management with regular ureteric stent exchanges every 3-4 months has successfully preserved renal function and improved his quality of life. Surgical closure was not pursued due to high operative risk, and repeat imaging has shown no evidence of persisting fistula, suggesting possible spontaneous closure. <b>Conclusion:</b> The treatment options for this ureteric small bowel fistula were limited. A lifelong nephrostomy was deemed unsuitable due to incompatibility with the patient's profession, and surgical intervention was associated with significant complexity due to the patient's history of malignancy and radiotherapy-related tissue changes. Therefore, a conservative strategy involving serial ureteric stent exchanges was pursued. Early recognition and individualised treatment of ureteric-enteric fistulas are essential, as timely intervention can significantly enhance prognosis and quality of life.</p>\",\"PeriodicalId\":30323,\"journal\":{\"name\":\"Case Reports in Urology\",\"volume\":\"2025 \",\"pages\":\"7232300\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12356682/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/criu/7232300\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/criu/7232300","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Management of Ureteric Small Bowel Fistula: A Case Report and Review of the Current Literature.
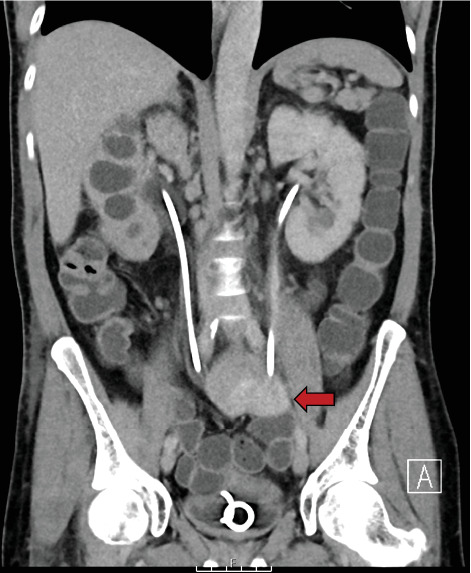
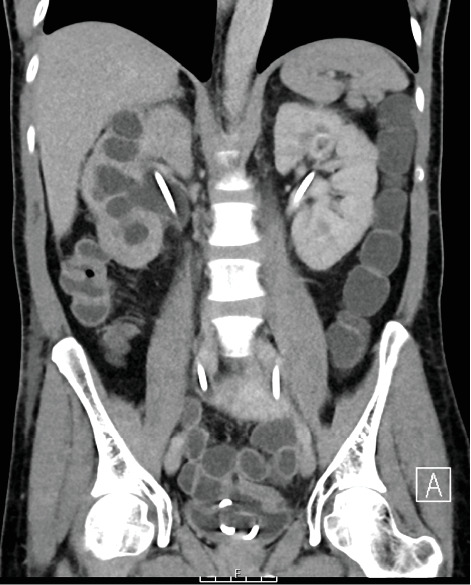
Background: Ureteric small bowel fistulas are rare entities, with limited reports in the literature. These pathological connections between the ureter and small bowel can lead to recurrent upper urinary tract infections and pose significant diagnostic and therapeutic challenges. The primary cause of ureteric small bowel fistula formation is iatrogenic intervention, such as percutaneous nephrolithotomy (PCNL) or abdominal surgery involving tissue resection. However, they can also arise spontaneously due to local chronic inflammation and infection. Given their rarity, there is no standardised management pathway, and the treatment approach should be individualised. Case Presentation: We present the case of a 57-year-old man presenting with a history of extensive locally advanced distal sigmoid carcinoma, managed with Hartmann's procedure with end colostomy followed by adjuvant radiotherapy and chemotherapy. He later developed a mid-ureteric small bowel fistula, presenting with urosepsis, a high-output stoma, deteriorating renal function and severe metabolic acidosis. Conservative management with regular ureteric stent exchanges every 3-4 months has successfully preserved renal function and improved his quality of life. Surgical closure was not pursued due to high operative risk, and repeat imaging has shown no evidence of persisting fistula, suggesting possible spontaneous closure. Conclusion: The treatment options for this ureteric small bowel fistula were limited. A lifelong nephrostomy was deemed unsuitable due to incompatibility with the patient's profession, and surgical intervention was associated with significant complexity due to the patient's history of malignancy and radiotherapy-related tissue changes. Therefore, a conservative strategy involving serial ureteric stent exchanges was pursued. Early recognition and individualised treatment of ureteric-enteric fistulas are essential, as timely intervention can significantly enhance prognosis and quality of life.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


