{"title":"全胃切除术后无症状脾梗死1例报告。","authors":"Atsuhito Takagi, Takashi Maeda, Satoshi Kobayashi, Atsushi Sekimura, Takehiro Takagi, Takuya Mishina, Yuya Hibino","doi":"10.70352/scrj.cr.25-0148","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Splenic infarction is a disease that develops as a result of a thrombotic predisposition. Most areas of malperfusion are usually small and unnoticeable. However, when massive infarction occurs, it is often diagnosed after the onset of clinical symptoms, such as abdominal pain or fever. In contrast, asymptomatic postoperative extensive splenic infarction is occasionally observed. Although conservative management is generally the first-line treatment for splenic infarction, surgical intervention is indicated in cases complicated by splenic abscess or rupture. Some reports suggest that extensive splenic infarction may result in atrophy or complete loss of the spleen over time.</p><p><strong>Case presentation: </strong>A 65-year-old woman presented with chronic epigastric pain and was diagnosed with gastric cancer through upper gastrointestinal endoscopy. The endoscopy revealed an ulcerated mass at the lesser curvature of the middle gastric body, and a biopsy confirmed a moderately differentiated adenocarcinoma. A laparoscopic distal gastrectomy was initially planned. However, the surgical approach was converted to an open total gastrectomy because of the spread of the tumor to the greater curvature of the gastric body and enlargement of the distal lymph nodes of the splenic artery, which were not included in the planned lymphadenectomy. Postoperatively, the patient experienced no abdominal pain or fever. However, on POD 7, blood tests revealed elevated hepatobiliary enzymes, and a contrast-enhanced CT (CECT) scan showed a loss of flow in the splenic artery and vein, leading to a diagnosis of extensive splenic infarction. A follow-up CECT scan 3 months later revealed a notable reduction of the splenic parenchyma over time.</p><p><strong>Conclusions: </strong>This is a rare case of asymptomatic, extensive splenic infarction incidentally diagnosed following total gastrectomy and successfully treated with conservative management.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12352957/pdf/","citationCount":"0","resultStr":"{\"title\":\"Asymptomatic Splenic Infarction Following Total Gastrectomy: A Case Report.\",\"authors\":\"Atsuhito Takagi, Takashi Maeda, Satoshi Kobayashi, Atsushi Sekimura, Takehiro Takagi, Takuya Mishina, Yuya Hibino\",\"doi\":\"10.70352/scrj.cr.25-0148\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Splenic infarction is a disease that develops as a result of a thrombotic predisposition. Most areas of malperfusion are usually small and unnoticeable. However, when massive infarction occurs, it is often diagnosed after the onset of clinical symptoms, such as abdominal pain or fever. In contrast, asymptomatic postoperative extensive splenic infarction is occasionally observed. Although conservative management is generally the first-line treatment for splenic infarction, surgical intervention is indicated in cases complicated by splenic abscess or rupture. Some reports suggest that extensive splenic infarction may result in atrophy or complete loss of the spleen over time.</p><p><strong>Case presentation: </strong>A 65-year-old woman presented with chronic epigastric pain and was diagnosed with gastric cancer through upper gastrointestinal endoscopy. The endoscopy revealed an ulcerated mass at the lesser curvature of the middle gastric body, and a biopsy confirmed a moderately differentiated adenocarcinoma. A laparoscopic distal gastrectomy was initially planned. However, the surgical approach was converted to an open total gastrectomy because of the spread of the tumor to the greater curvature of the gastric body and enlargement of the distal lymph nodes of the splenic artery, which were not included in the planned lymphadenectomy. Postoperatively, the patient experienced no abdominal pain or fever. However, on POD 7, blood tests revealed elevated hepatobiliary enzymes, and a contrast-enhanced CT (CECT) scan showed a loss of flow in the splenic artery and vein, leading to a diagnosis of extensive splenic infarction. A follow-up CECT scan 3 months later revealed a notable reduction of the splenic parenchyma over time.</p><p><strong>Conclusions: </strong>This is a rare case of asymptomatic, extensive splenic infarction incidentally diagnosed following total gastrectomy and successfully treated with conservative management.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12352957/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0148\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0148","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/14 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Asymptomatic Splenic Infarction Following Total Gastrectomy: A Case Report.
Introduction: Splenic infarction is a disease that develops as a result of a thrombotic predisposition. Most areas of malperfusion are usually small and unnoticeable. However, when massive infarction occurs, it is often diagnosed after the onset of clinical symptoms, such as abdominal pain or fever. In contrast, asymptomatic postoperative extensive splenic infarction is occasionally observed. Although conservative management is generally the first-line treatment for splenic infarction, surgical intervention is indicated in cases complicated by splenic abscess or rupture. Some reports suggest that extensive splenic infarction may result in atrophy or complete loss of the spleen over time.
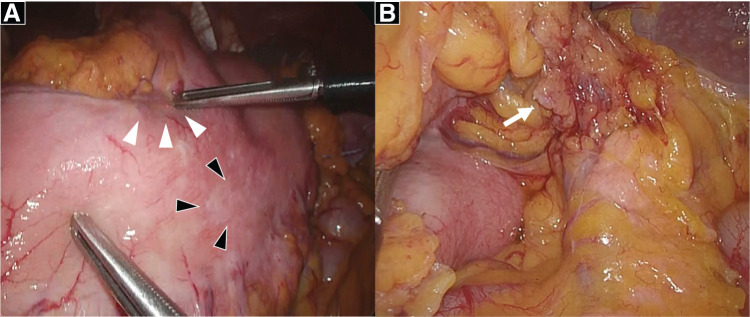
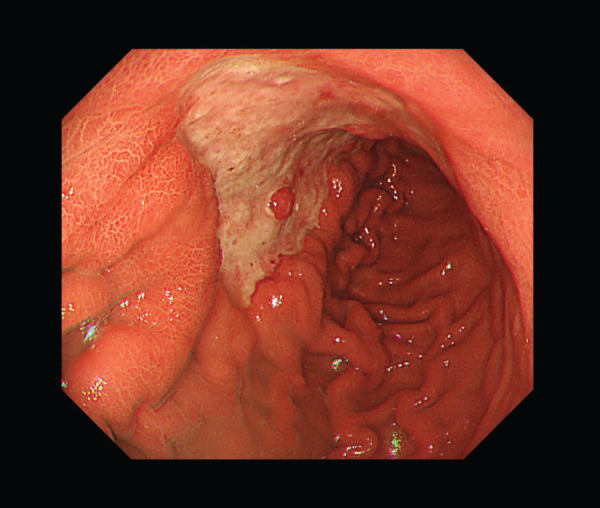
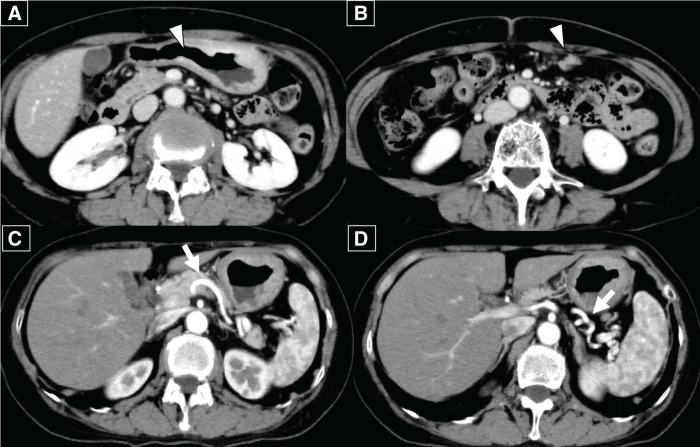
Case presentation: A 65-year-old woman presented with chronic epigastric pain and was diagnosed with gastric cancer through upper gastrointestinal endoscopy. The endoscopy revealed an ulcerated mass at the lesser curvature of the middle gastric body, and a biopsy confirmed a moderately differentiated adenocarcinoma. A laparoscopic distal gastrectomy was initially planned. However, the surgical approach was converted to an open total gastrectomy because of the spread of the tumor to the greater curvature of the gastric body and enlargement of the distal lymph nodes of the splenic artery, which were not included in the planned lymphadenectomy. Postoperatively, the patient experienced no abdominal pain or fever. However, on POD 7, blood tests revealed elevated hepatobiliary enzymes, and a contrast-enhanced CT (CECT) scan showed a loss of flow in the splenic artery and vein, leading to a diagnosis of extensive splenic infarction. A follow-up CECT scan 3 months later revealed a notable reduction of the splenic parenchyma over time.
Conclusions: This is a rare case of asymptomatic, extensive splenic infarction incidentally diagnosed following total gastrectomy and successfully treated with conservative management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


