{"title":"应激高血糖比和血红蛋白与RDW比预测溶栓治疗卒中的预后:一项回顾性队列研究。","authors":"Sarawut Krongsut, Nat Na-Ek","doi":"10.22037/aaemj.v13i1.2730","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>High stress hyperglycemia ratio (SHR) and low hemoglobin-to-red blood cell distribution width ratio (HB/RDW) are each known predictors of mortality in acute ischemic stroke (AIS). This study aimed to assess the predictive performance of high SHR (≥1.18) and low HB/RDW (≤0.76) together in stroke patients treated with thrombolysis.</p><p><strong>Methods: </strong>We retrospectively collected data from 345 AIS patients treated with thrombolysis. HB/RDW values were obtained from pre-recombinant tissue plasminogen activator complete blood counts; while fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) levels were measured in the morning after an 8-14-hour overnight fast. Patients were categorized into four groups based on SHR and HB/RDW levels. We used multivariable Poisson regression with robust variance to estimate risk ratios (RRs) and 95% confidence intervals (CIs). Models assessed associations with in-hospital mortality (IHM), early neurological deterioration (END), and functional outcomes at discharge and 3 months, adjusting for age, sex, prior stroke, pre-existing disability, myocardial infarction, atrial fibrillation, heart failure, chronic kidney disease, and malignancy. Propensity score weighting analysis was further conducted as a sensitivity analysis.</p><p><strong>Results: </strong>Among 345 patients, only 37 were in the high SHR (SHR+) and low HB/RDW (HB/RDW+) group. A total of 65 patients (18.8%) died during hospitalization. The SHR+ HB/RDW+ group had significantly higher risks of IHM (adjusted RR: 9.97, 95% CI: 4.95-20.08), END (adjusted RR: 2.95, 95% CI: 1.51-5.77), 3-month mortality (adjusted RR: 6.23, 95% CI: 3.49-11.12), and poor 3-month functional outcomes (adjusted RR: 2.86, 95% CI: 2.01-4.06) compared to the SHR- HB/RDW- group. These associations remained robust across sensitivity analyses. The combination of SHR ≥1.18 and HB/RDW ≤0.76 predicted IHM with an AuROC of 0.78 (95% CI: 0.73-0.83). Although the combined biomarker improved sensitivity and net benefit, its AUROC was not statistically superior to that of individual markers.</p><p><strong>Conclusions: </strong>Combined high SHR and low HB/RDW levels at admission significantly predict poor outcomes in thrombolysis-treated AIS, performing better than either biomarker alone. Further validation in larger, diverse cohorts is warranted.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e65"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12341010/pdf/","citationCount":"0","resultStr":"{\"title\":\"Stress Hyperglycemia Ratio and Hemoglobin to RDW Ratio in Predicting the Outcomes of Thrombolysis-Treated Stroke: A Retrospective Cohort Study.\",\"authors\":\"Sarawut Krongsut, Nat Na-Ek\",\"doi\":\"10.22037/aaemj.v13i1.2730\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>High stress hyperglycemia ratio (SHR) and low hemoglobin-to-red blood cell distribution width ratio (HB/RDW) are each known predictors of mortality in acute ischemic stroke (AIS). This study aimed to assess the predictive performance of high SHR (≥1.18) and low HB/RDW (≤0.76) together in stroke patients treated with thrombolysis.</p><p><strong>Methods: </strong>We retrospectively collected data from 345 AIS patients treated with thrombolysis. HB/RDW values were obtained from pre-recombinant tissue plasminogen activator complete blood counts; while fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) levels were measured in the morning after an 8-14-hour overnight fast. Patients were categorized into four groups based on SHR and HB/RDW levels. We used multivariable Poisson regression with robust variance to estimate risk ratios (RRs) and 95% confidence intervals (CIs). Models assessed associations with in-hospital mortality (IHM), early neurological deterioration (END), and functional outcomes at discharge and 3 months, adjusting for age, sex, prior stroke, pre-existing disability, myocardial infarction, atrial fibrillation, heart failure, chronic kidney disease, and malignancy. Propensity score weighting analysis was further conducted as a sensitivity analysis.</p><p><strong>Results: </strong>Among 345 patients, only 37 were in the high SHR (SHR+) and low HB/RDW (HB/RDW+) group. A total of 65 patients (18.8%) died during hospitalization. The SHR+ HB/RDW+ group had significantly higher risks of IHM (adjusted RR: 9.97, 95% CI: 4.95-20.08), END (adjusted RR: 2.95, 95% CI: 1.51-5.77), 3-month mortality (adjusted RR: 6.23, 95% CI: 3.49-11.12), and poor 3-month functional outcomes (adjusted RR: 2.86, 95% CI: 2.01-4.06) compared to the SHR- HB/RDW- group. These associations remained robust across sensitivity analyses. The combination of SHR ≥1.18 and HB/RDW ≤0.76 predicted IHM with an AuROC of 0.78 (95% CI: 0.73-0.83). Although the combined biomarker improved sensitivity and net benefit, its AUROC was not statistically superior to that of individual markers.</p><p><strong>Conclusions: </strong>Combined high SHR and low HB/RDW levels at admission significantly predict poor outcomes in thrombolysis-treated AIS, performing better than either biomarker alone. Further validation in larger, diverse cohorts is warranted.</p>\",\"PeriodicalId\":8146,\"journal\":{\"name\":\"Archives of Academic Emergency Medicine\",\"volume\":\"13 1\",\"pages\":\"e65\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12341010/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Academic Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22037/aaemj.v13i1.2730\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2730","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Stress Hyperglycemia Ratio and Hemoglobin to RDW Ratio in Predicting the Outcomes of Thrombolysis-Treated Stroke: A Retrospective Cohort Study.
Introduction: High stress hyperglycemia ratio (SHR) and low hemoglobin-to-red blood cell distribution width ratio (HB/RDW) are each known predictors of mortality in acute ischemic stroke (AIS). This study aimed to assess the predictive performance of high SHR (≥1.18) and low HB/RDW (≤0.76) together in stroke patients treated with thrombolysis.
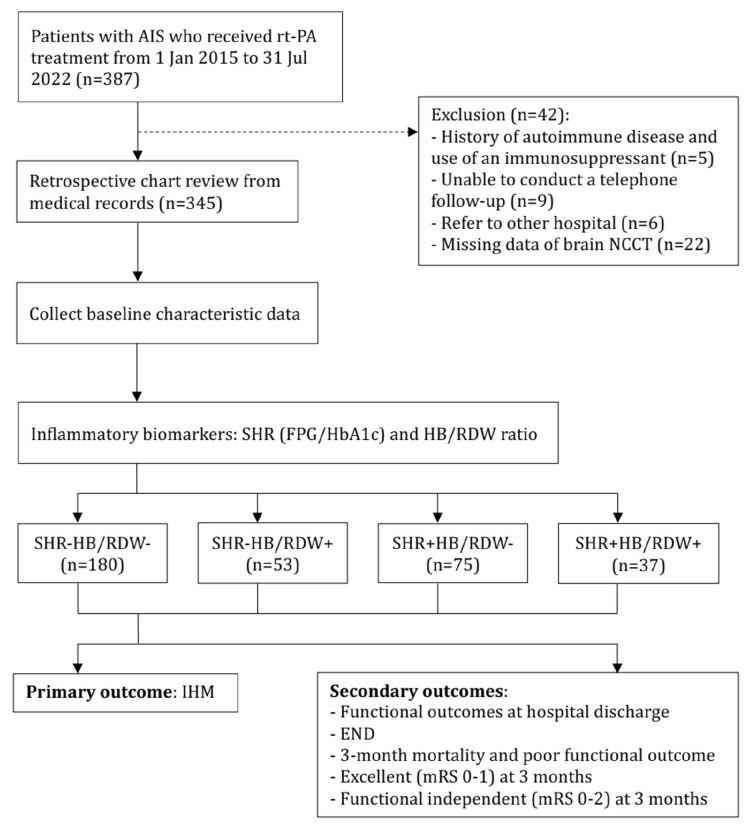
Methods: We retrospectively collected data from 345 AIS patients treated with thrombolysis. HB/RDW values were obtained from pre-recombinant tissue plasminogen activator complete blood counts; while fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) levels were measured in the morning after an 8-14-hour overnight fast. Patients were categorized into four groups based on SHR and HB/RDW levels. We used multivariable Poisson regression with robust variance to estimate risk ratios (RRs) and 95% confidence intervals (CIs). Models assessed associations with in-hospital mortality (IHM), early neurological deterioration (END), and functional outcomes at discharge and 3 months, adjusting for age, sex, prior stroke, pre-existing disability, myocardial infarction, atrial fibrillation, heart failure, chronic kidney disease, and malignancy. Propensity score weighting analysis was further conducted as a sensitivity analysis.
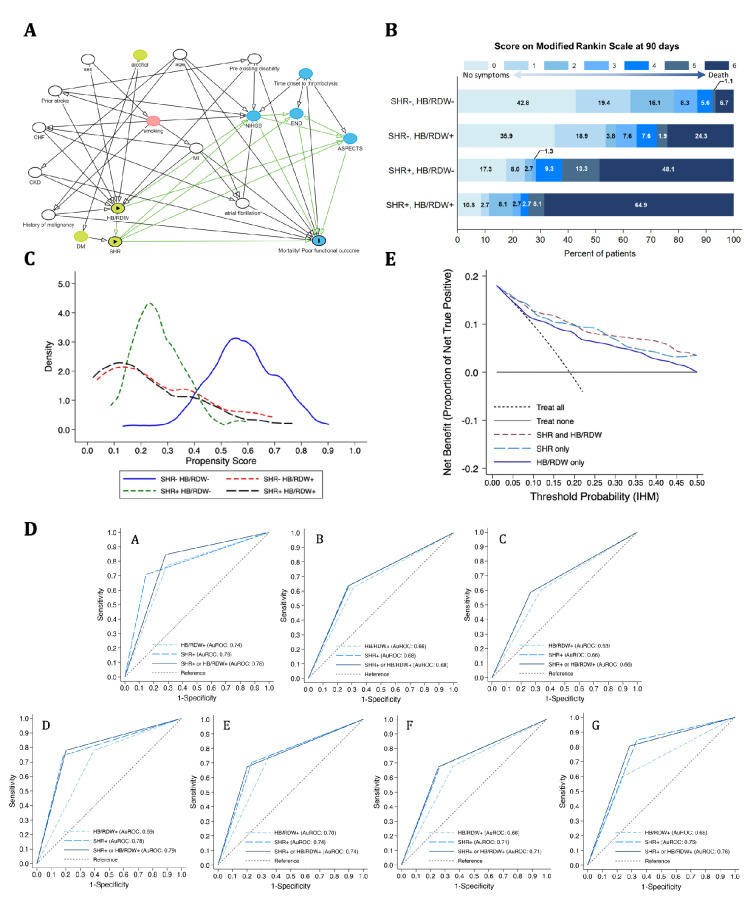
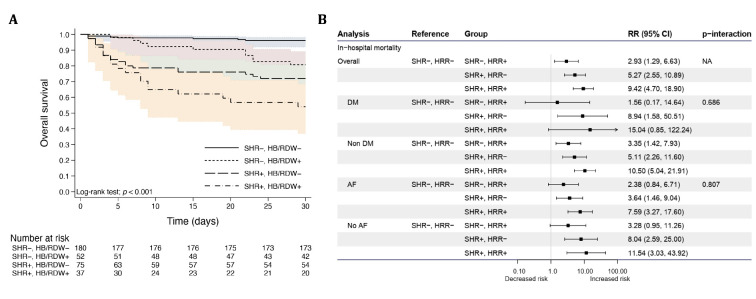
Results: Among 345 patients, only 37 were in the high SHR (SHR+) and low HB/RDW (HB/RDW+) group. A total of 65 patients (18.8%) died during hospitalization. The SHR+ HB/RDW+ group had significantly higher risks of IHM (adjusted RR: 9.97, 95% CI: 4.95-20.08), END (adjusted RR: 2.95, 95% CI: 1.51-5.77), 3-month mortality (adjusted RR: 6.23, 95% CI: 3.49-11.12), and poor 3-month functional outcomes (adjusted RR: 2.86, 95% CI: 2.01-4.06) compared to the SHR- HB/RDW- group. These associations remained robust across sensitivity analyses. The combination of SHR ≥1.18 and HB/RDW ≤0.76 predicted IHM with an AuROC of 0.78 (95% CI: 0.73-0.83). Although the combined biomarker improved sensitivity and net benefit, its AUROC was not statistically superior to that of individual markers.
Conclusions: Combined high SHR and low HB/RDW levels at admission significantly predict poor outcomes in thrombolysis-treated AIS, performing better than either biomarker alone. Further validation in larger, diverse cohorts is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


