Moazzam Shahzad, Muhammad Kashif Amin, Maggie Nelson, Abhinav Vyas, Joe S Al-Ramahi, Nausheen Ahmed, Rajat Bansal, Haitham Abdelhakim, Leyla Shune, Al-Ola Abdallah, Anurag K Singh, Sunil H Abhyankar, Joseph P McGuirk, Muhammad Umair Mushtaq
{"title":"同时静脉输注免疫球蛋白和血小板治疗同种异体造血干细胞移植患者难治性同种免疫血小板减少症。","authors":"Moazzam Shahzad, Muhammad Kashif Amin, Maggie Nelson, Abhinav Vyas, Joe S Al-Ramahi, Nausheen Ahmed, Rajat Bansal, Haitham Abdelhakim, Leyla Shune, Al-Ola Abdallah, Anurag K Singh, Sunil H Abhyankar, Joseph P McGuirk, Muhammad Umair Mushtaq","doi":"10.1016/j.htct.2025.103961","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Severe refractory alloimmune thrombocytopenia is a challenging and life-threatening complication in patients with hematologic disorders who are undergoing allogeneic hematopoietic stem cell transplantation. This study aimed to investigate the utility of continuous intravenous immunoglobulin and platelet transfusions as a therapeutic approach for alloimmune thrombocytopenia in patients undergoing allogeneic transplants.</p><p><strong>Methods: </strong>A single-center retrospective analysis was conducted of ten adult allogeneic transplant patients hospitalized with transfusion-refractory alloimmune thrombocytopenia. Intravenous immunoglobulin (2 g/kg) was administered as a slow continuous infusion over 48 h along with a continuous apheresis platelet infusion (one apheresis unit over eight hours). Clinical response was defined as the resolution of bleeding or patients being able to undergo the required procedure without bleeding complications.</p><p><strong>Results: </strong>The median time after the transplant was 27.5 (range: 7-299) days. Myeloablative and reduced-intensity conditioning were performed in 5 (50 %) and 5 (50 %) patients, respectively. The median platelet count at the time of infusion was 4.5 × 10<sup>9</sup>/L. All patients were able to achieve clinical response with the median maximum platelet count within ten days of the infusion being 41.0 × 10<sup>9</sup>/L. The median time to best response was three days with a median platelet count of 27.0 × 10⁹/L.</p><p><strong>Conclusions: </strong>Continuous intravenous immunoglobulin and platelet infusions over 48 h may be able to overcome life-threatening refractory alloimmune thrombocytopenia in transplant patients and may provide a bridging measure until platelet engraftment or for life-threatening hemorrhage or invasive procedures with high bleeding risk.</p>","PeriodicalId":94026,"journal":{"name":"Hematology, transfusion and cell therapy","volume":"47 4","pages":"103961"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12356998/pdf/","citationCount":"0","resultStr":"{\"title\":\"Concurrent intravenous immunoglobulin and platelet transfusion for refractory alloimmune thrombocytopenia in patients undergoing allogeneic hematopoietic stem cell transplantation.\",\"authors\":\"Moazzam Shahzad, Muhammad Kashif Amin, Maggie Nelson, Abhinav Vyas, Joe S Al-Ramahi, Nausheen Ahmed, Rajat Bansal, Haitham Abdelhakim, Leyla Shune, Al-Ola Abdallah, Anurag K Singh, Sunil H Abhyankar, Joseph P McGuirk, Muhammad Umair Mushtaq\",\"doi\":\"10.1016/j.htct.2025.103961\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Severe refractory alloimmune thrombocytopenia is a challenging and life-threatening complication in patients with hematologic disorders who are undergoing allogeneic hematopoietic stem cell transplantation. This study aimed to investigate the utility of continuous intravenous immunoglobulin and platelet transfusions as a therapeutic approach for alloimmune thrombocytopenia in patients undergoing allogeneic transplants.</p><p><strong>Methods: </strong>A single-center retrospective analysis was conducted of ten adult allogeneic transplant patients hospitalized with transfusion-refractory alloimmune thrombocytopenia. Intravenous immunoglobulin (2 g/kg) was administered as a slow continuous infusion over 48 h along with a continuous apheresis platelet infusion (one apheresis unit over eight hours). Clinical response was defined as the resolution of bleeding or patients being able to undergo the required procedure without bleeding complications.</p><p><strong>Results: </strong>The median time after the transplant was 27.5 (range: 7-299) days. Myeloablative and reduced-intensity conditioning were performed in 5 (50 %) and 5 (50 %) patients, respectively. The median platelet count at the time of infusion was 4.5 × 10<sup>9</sup>/L. All patients were able to achieve clinical response with the median maximum platelet count within ten days of the infusion being 41.0 × 10<sup>9</sup>/L. The median time to best response was three days with a median platelet count of 27.0 × 10⁹/L.</p><p><strong>Conclusions: </strong>Continuous intravenous immunoglobulin and platelet infusions over 48 h may be able to overcome life-threatening refractory alloimmune thrombocytopenia in transplant patients and may provide a bridging measure until platelet engraftment or for life-threatening hemorrhage or invasive procedures with high bleeding risk.</p>\",\"PeriodicalId\":94026,\"journal\":{\"name\":\"Hematology, transfusion and cell therapy\",\"volume\":\"47 4\",\"pages\":\"103961\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12356998/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematology, transfusion and cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/j.htct.2025.103961\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology, transfusion and cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.htct.2025.103961","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Concurrent intravenous immunoglobulin and platelet transfusion for refractory alloimmune thrombocytopenia in patients undergoing allogeneic hematopoietic stem cell transplantation.
Background: Severe refractory alloimmune thrombocytopenia is a challenging and life-threatening complication in patients with hematologic disorders who are undergoing allogeneic hematopoietic stem cell transplantation. This study aimed to investigate the utility of continuous intravenous immunoglobulin and platelet transfusions as a therapeutic approach for alloimmune thrombocytopenia in patients undergoing allogeneic transplants.
Methods: A single-center retrospective analysis was conducted of ten adult allogeneic transplant patients hospitalized with transfusion-refractory alloimmune thrombocytopenia. Intravenous immunoglobulin (2 g/kg) was administered as a slow continuous infusion over 48 h along with a continuous apheresis platelet infusion (one apheresis unit over eight hours). Clinical response was defined as the resolution of bleeding or patients being able to undergo the required procedure without bleeding complications.
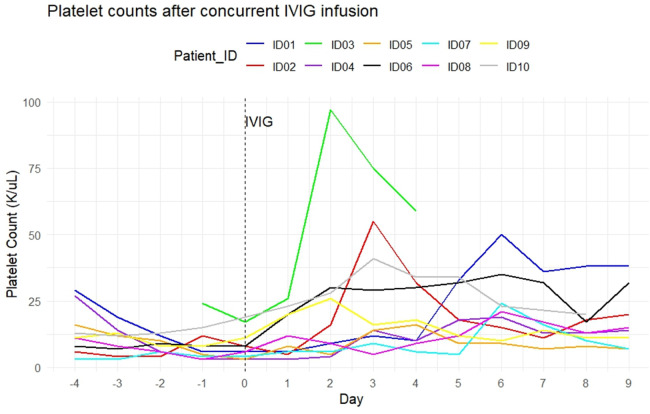
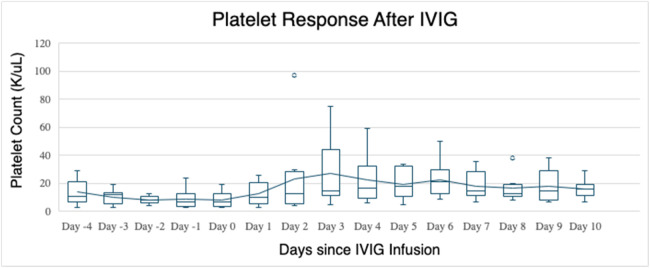
Results: The median time after the transplant was 27.5 (range: 7-299) days. Myeloablative and reduced-intensity conditioning were performed in 5 (50 %) and 5 (50 %) patients, respectively. The median platelet count at the time of infusion was 4.5 × 109/L. All patients were able to achieve clinical response with the median maximum platelet count within ten days of the infusion being 41.0 × 109/L. The median time to best response was three days with a median platelet count of 27.0 × 10⁹/L.
Conclusions: Continuous intravenous immunoglobulin and platelet infusions over 48 h may be able to overcome life-threatening refractory alloimmune thrombocytopenia in transplant patients and may provide a bridging measure until platelet engraftment or for life-threatening hemorrhage or invasive procedures with high bleeding risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


