{"title":"角膜神经化与COVID-19相遇:微创角膜神经化合并COVID-19相关性角膜炎1例","authors":"Shuqin Zhuang, Qiaoran Qi, Jiaying Zhang, Jin Li","doi":"10.1186/s12348-025-00521-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To report a rare case of severe keratitis followed by SARS-CoV-2 infection after minimally invasive corneal neurotization (MICN) surgery for the first time.</p><p><strong>Methods: </strong>Retrospective single case report.</p><p><strong>Results: </strong>A 59-year-old female presented to ophthalmology department of our hospital with facial paralysis induced by neurosurgeries. After detailed ophthalmological examination, she was diagnosed with Mackie stage III neurotrophic keratopathy (NK) in the right eye and subsequently underwent MICN and amniotic membrane transplantation. Postoperatively, corneal sensation and the epithelial defect showed gradual improvement, with corneal sensation recovering to 30 mm (measured by Cochet-Bonnet esthesiometer). However, thirteen months after MICN, she developed a corneal ulcer in the right eye one week after contracting SARS-CoV-2 (COVID-19). Supplementary investigations, including anterior segment photography, in vivo confocal microscopy (IVCM), and corneal scraping for pathogen detection, revealed recurrent corneal anesthesia and loss of corneal nerves, with no pathogens identified. After two weeks of empirical antiviral and antibacterial therapy yielded no significant improvement, a diagnosis of COVID-19-induced neurotrophic keratitis (Stage III Mackie) was established. Management consisted of prolonged medical therapy (including antiviral agents, antibiotics, nutritional supplementation, corticosteroids, and artificial tears), two amniotic membrane transplants, and one temporary tarsorrhaphy. Following two years of treatment and follow-up, the corneal lesion achieved complete healing with corneal nerve regeneration and restoration of corneal sensation.</p><p><strong>Conclusion: </strong>This study presents the first documented case of COVID-19-related NK following MICN established as a diagnosis of exclusion. This case underscores the critical need for comprehensive differential diagnosis to rule out infectious etiologies in post-MICN keratitis, ultimately leading to a diagnosis of exclusion for COVID-19-induced disease. The diagnostic approach outlined may offer valuable insights for similar presentations. After a protracted clinical course, the patient ultimately achieved restoration of corneal sensation and reinnervation, demonstrating the preserved regenerative potential of MICN-reconstructed neural pathways even after severe viral infection.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"15 1","pages":"60"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335426/pdf/","citationCount":"0","resultStr":"{\"title\":\"Corneal neurotization meets COVID-19: a case report of minimally invasive corneal neurotization complicated by COVID-19-related keratitis.\",\"authors\":\"Shuqin Zhuang, Qiaoran Qi, Jiaying Zhang, Jin Li\",\"doi\":\"10.1186/s12348-025-00521-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To report a rare case of severe keratitis followed by SARS-CoV-2 infection after minimally invasive corneal neurotization (MICN) surgery for the first time.</p><p><strong>Methods: </strong>Retrospective single case report.</p><p><strong>Results: </strong>A 59-year-old female presented to ophthalmology department of our hospital with facial paralysis induced by neurosurgeries. After detailed ophthalmological examination, she was diagnosed with Mackie stage III neurotrophic keratopathy (NK) in the right eye and subsequently underwent MICN and amniotic membrane transplantation. Postoperatively, corneal sensation and the epithelial defect showed gradual improvement, with corneal sensation recovering to 30 mm (measured by Cochet-Bonnet esthesiometer). However, thirteen months after MICN, she developed a corneal ulcer in the right eye one week after contracting SARS-CoV-2 (COVID-19). Supplementary investigations, including anterior segment photography, in vivo confocal microscopy (IVCM), and corneal scraping for pathogen detection, revealed recurrent corneal anesthesia and loss of corneal nerves, with no pathogens identified. After two weeks of empirical antiviral and antibacterial therapy yielded no significant improvement, a diagnosis of COVID-19-induced neurotrophic keratitis (Stage III Mackie) was established. Management consisted of prolonged medical therapy (including antiviral agents, antibiotics, nutritional supplementation, corticosteroids, and artificial tears), two amniotic membrane transplants, and one temporary tarsorrhaphy. Following two years of treatment and follow-up, the corneal lesion achieved complete healing with corneal nerve regeneration and restoration of corneal sensation.</p><p><strong>Conclusion: </strong>This study presents the first documented case of COVID-19-related NK following MICN established as a diagnosis of exclusion. This case underscores the critical need for comprehensive differential diagnosis to rule out infectious etiologies in post-MICN keratitis, ultimately leading to a diagnosis of exclusion for COVID-19-induced disease. The diagnostic approach outlined may offer valuable insights for similar presentations. After a protracted clinical course, the patient ultimately achieved restoration of corneal sensation and reinnervation, demonstrating the preserved regenerative potential of MICN-reconstructed neural pathways even after severe viral infection.</p>\",\"PeriodicalId\":16600,\"journal\":{\"name\":\"Journal of Ophthalmic Inflammation and Infection\",\"volume\":\"15 1\",\"pages\":\"60\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335426/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Ophthalmic Inflammation and Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s12348-025-00521-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-025-00521-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:报道一例罕见的微创角膜神经化(MICN)术后严重角膜炎并发SARS-CoV-2感染。方法:单例回顾性报告。结果:1例59岁女性因神经外科手术所致面瘫就诊于我院眼科。经过详细的眼科检查,她被诊断为右眼Mackie III期神经营养性角膜病变(NK),随后接受了MICN和羊膜移植。术后角膜感觉和上皮缺损逐渐改善,角膜感觉恢复至30 mm (Cochet-Bonnet感觉计测量)。然而,在MICN后13个月,她在感染SARS-CoV-2 (COVID-19)一周后右眼出现角膜溃疡。补充调查,包括前段摄影、体内共聚焦显微镜(IVCM)和角膜刮痧进行病原体检测,发现复发性角膜麻醉和角膜神经丧失,未发现病原体。经过两周的经验性抗病毒和抗菌治疗,没有明显改善,诊断为covid -19诱导的神经营养性角膜炎(III期Mackie)。治疗包括长期药物治疗(包括抗病毒药物、抗生素、营养补充、皮质类固醇和人工泪液)、两次羊膜移植和一次临时缝合术。经过2年的治疗和随访,角膜病变完全愈合,角膜神经再生,角膜感觉恢复。结论:本研究报道了首例记录在案的covid -19相关NK病例,MICN被确定为排除诊断。该病例强调了全面鉴别诊断的迫切需要,以排除micn后角膜炎的感染病因,最终导致排除covid -19诱导疾病的诊断。概述的诊断方法可能为类似的演示提供有价值的见解。经过漫长的临床过程,患者最终实现了角膜感觉和神经再生的恢复,这表明即使在严重的病毒感染后,micn重建的神经通路也保留了再生潜力。
Corneal neurotization meets COVID-19: a case report of minimally invasive corneal neurotization complicated by COVID-19-related keratitis.
Purpose: To report a rare case of severe keratitis followed by SARS-CoV-2 infection after minimally invasive corneal neurotization (MICN) surgery for the first time.
Methods: Retrospective single case report.
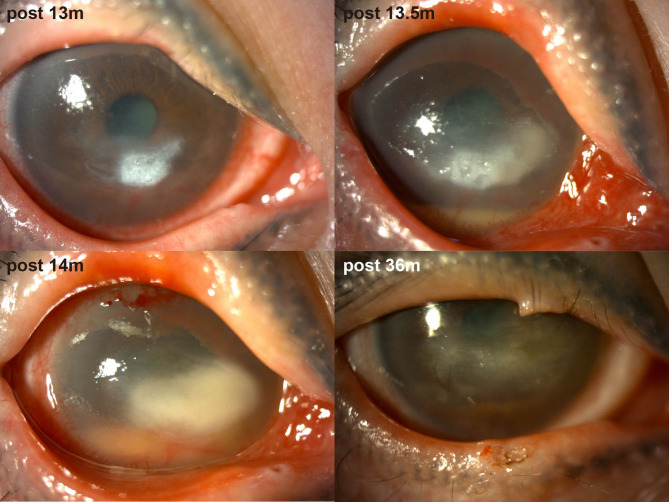
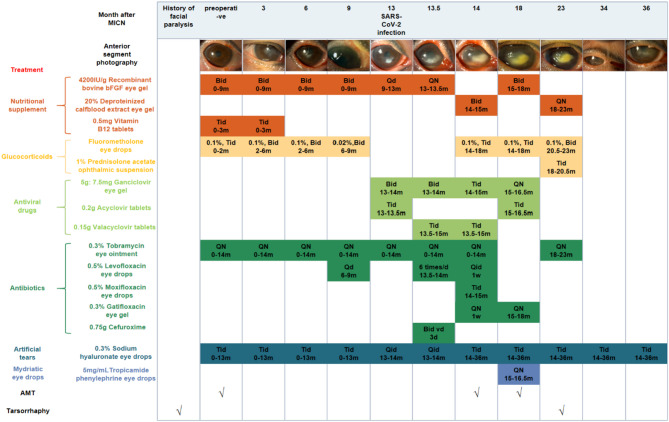
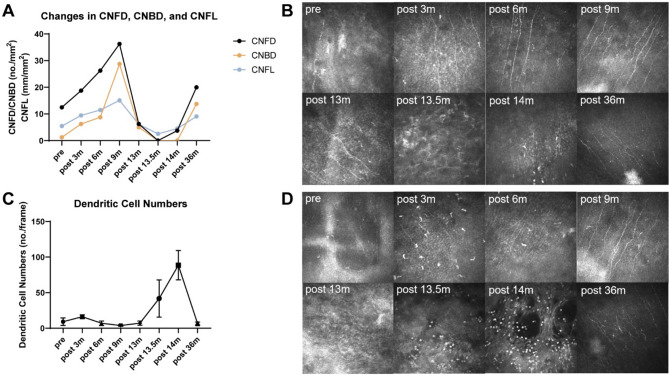
Results: A 59-year-old female presented to ophthalmology department of our hospital with facial paralysis induced by neurosurgeries. After detailed ophthalmological examination, she was diagnosed with Mackie stage III neurotrophic keratopathy (NK) in the right eye and subsequently underwent MICN and amniotic membrane transplantation. Postoperatively, corneal sensation and the epithelial defect showed gradual improvement, with corneal sensation recovering to 30 mm (measured by Cochet-Bonnet esthesiometer). However, thirteen months after MICN, she developed a corneal ulcer in the right eye one week after contracting SARS-CoV-2 (COVID-19). Supplementary investigations, including anterior segment photography, in vivo confocal microscopy (IVCM), and corneal scraping for pathogen detection, revealed recurrent corneal anesthesia and loss of corneal nerves, with no pathogens identified. After two weeks of empirical antiviral and antibacterial therapy yielded no significant improvement, a diagnosis of COVID-19-induced neurotrophic keratitis (Stage III Mackie) was established. Management consisted of prolonged medical therapy (including antiviral agents, antibiotics, nutritional supplementation, corticosteroids, and artificial tears), two amniotic membrane transplants, and one temporary tarsorrhaphy. Following two years of treatment and follow-up, the corneal lesion achieved complete healing with corneal nerve regeneration and restoration of corneal sensation.
Conclusion: This study presents the first documented case of COVID-19-related NK following MICN established as a diagnosis of exclusion. This case underscores the critical need for comprehensive differential diagnosis to rule out infectious etiologies in post-MICN keratitis, ultimately leading to a diagnosis of exclusion for COVID-19-induced disease. The diagnostic approach outlined may offer valuable insights for similar presentations. After a protracted clinical course, the patient ultimately achieved restoration of corneal sensation and reinnervation, demonstrating the preserved regenerative potential of MICN-reconstructed neural pathways even after severe viral infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


