Harshit Arora, Hassan Darabi, Nathaniel Toop, Amy Minnema, Zahraa Al-Sharshahi, Grace M Martin, Kelsey Karnik, Jan M Schwab, Francis Farhadi
{"title":"脊髓肿胀和硬膜内压迫预测急性颈外伤性脊髓损伤后神经恢复。","authors":"Harshit Arora, Hassan Darabi, Nathaniel Toop, Amy Minnema, Zahraa Al-Sharshahi, Grace M Martin, Kelsey Karnik, Jan M Schwab, Francis Farhadi","doi":"10.1371/journal.pone.0325827","DOIUrl":null,"url":null,"abstract":"<p><p>Intradural spinal cord compression impairs perfusion pressure and is putatively rate-limiting for recovery after traumatic spinal cord injury (tSCI). After cervical tSCI, even minimally improved tissue preservation may help promote neurological recovery. To assess the nature and extent of spinal cord swelling and compression post-acute cervical tSCI, we evaluated several baseline MRI parameters including BASIC score, intramedullary lesion (IML) length, maximal canal compromise (MCC), maximal spinal cord compression (MSCC), extent of cord compression (ECC), maximal swollen anteroposterior diameter adjacent to injury site (Dmax), and maximal cord swelling (MCS) in 169 consecutive patients across 2 centers. In patients with either primarily intradural or combined (MSCC ≤5% or >5%, respectively) cord compression, we examined the predictive value of clinical and imaging admission parameters on American Spinal Injury Association Impairment Scale (AIS) severity and conversion up to 1-year follow-up. 37 (21.9%) patients presented with primarily intradural while 132 (78.1%) had combined cord compression. MSCC, MCS, and Dmax values differed significantly between the two groups (p < 0.0001, < 0.01 and < 0.001, respectively). MSCC was associated with age, MCC and MCS at baseline, while MCS was associated with age, MSCC and Dmax, on multivariable analysis. Logistic regression analysis of areas under receiver operating characteristic curve (AUROC) confirmed ECC (AUC 0.678) and MCS (AUC 0.922) as good and excellent predictors, respectively of AIS-conversion at 1-year for intradural compression participants. Additionally, MCS was significantly more accurate in predicting AIS-conversion in intradural group and the probability of AIS-conversion significantly decreased with each 1% increase in MCS (p = 0.003; OR 0.949), for both compression subtypes. In conclusion, baseline measures of cord swelling predict AIS-conversion likelihood up to 1-year. The deleterious effects of intradural cord compression, either isolated or presenting with extradural compression, may benefit from supplemental decompression strategies in addition to current standard-of-care.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 8","pages":"e0325827"},"PeriodicalIF":2.6000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331075/pdf/","citationCount":"0","resultStr":"{\"title\":\"Spinal cord swelling and intradural compression predict neurological recovery after acute cervical traumatic spinal cord injury.\",\"authors\":\"Harshit Arora, Hassan Darabi, Nathaniel Toop, Amy Minnema, Zahraa Al-Sharshahi, Grace M Martin, Kelsey Karnik, Jan M Schwab, Francis Farhadi\",\"doi\":\"10.1371/journal.pone.0325827\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Intradural spinal cord compression impairs perfusion pressure and is putatively rate-limiting for recovery after traumatic spinal cord injury (tSCI). After cervical tSCI, even minimally improved tissue preservation may help promote neurological recovery. To assess the nature and extent of spinal cord swelling and compression post-acute cervical tSCI, we evaluated several baseline MRI parameters including BASIC score, intramedullary lesion (IML) length, maximal canal compromise (MCC), maximal spinal cord compression (MSCC), extent of cord compression (ECC), maximal swollen anteroposterior diameter adjacent to injury site (Dmax), and maximal cord swelling (MCS) in 169 consecutive patients across 2 centers. In patients with either primarily intradural or combined (MSCC ≤5% or >5%, respectively) cord compression, we examined the predictive value of clinical and imaging admission parameters on American Spinal Injury Association Impairment Scale (AIS) severity and conversion up to 1-year follow-up. 37 (21.9%) patients presented with primarily intradural while 132 (78.1%) had combined cord compression. MSCC, MCS, and Dmax values differed significantly between the two groups (p < 0.0001, < 0.01 and < 0.001, respectively). MSCC was associated with age, MCC and MCS at baseline, while MCS was associated with age, MSCC and Dmax, on multivariable analysis. Logistic regression analysis of areas under receiver operating characteristic curve (AUROC) confirmed ECC (AUC 0.678) and MCS (AUC 0.922) as good and excellent predictors, respectively of AIS-conversion at 1-year for intradural compression participants. Additionally, MCS was significantly more accurate in predicting AIS-conversion in intradural group and the probability of AIS-conversion significantly decreased with each 1% increase in MCS (p = 0.003; OR 0.949), for both compression subtypes. In conclusion, baseline measures of cord swelling predict AIS-conversion likelihood up to 1-year. The deleterious effects of intradural cord compression, either isolated or presenting with extradural compression, may benefit from supplemental decompression strategies in addition to current standard-of-care.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 8\",\"pages\":\"e0325827\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331075/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0325827\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0325827","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Spinal cord swelling and intradural compression predict neurological recovery after acute cervical traumatic spinal cord injury.
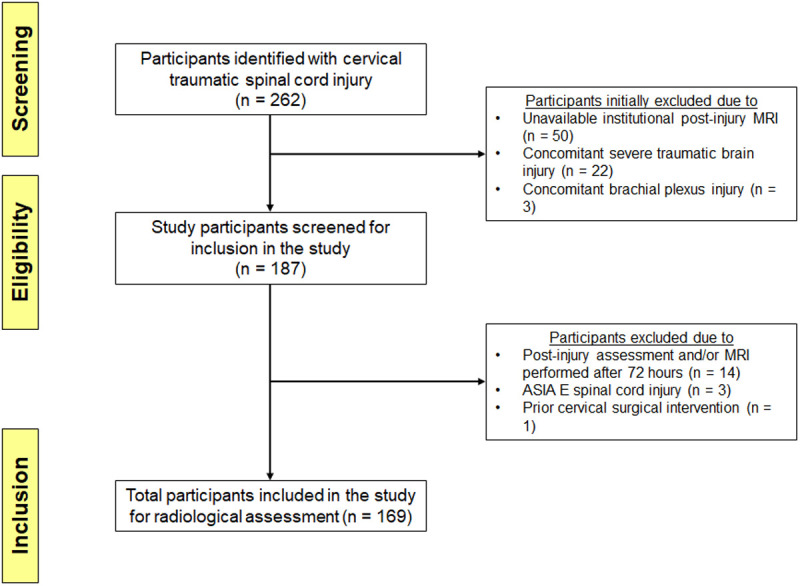
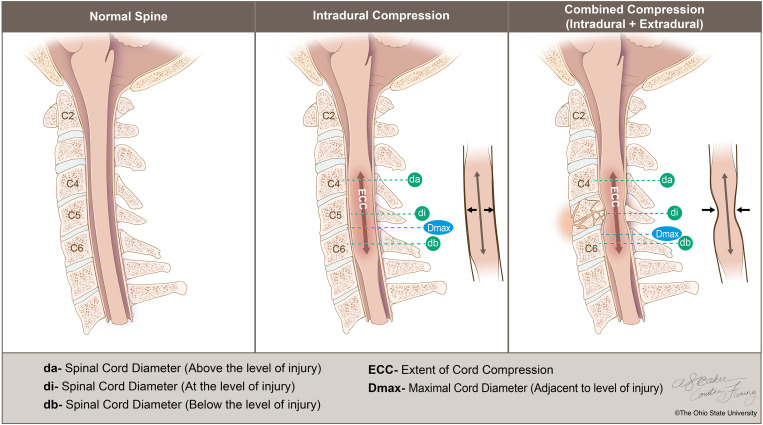
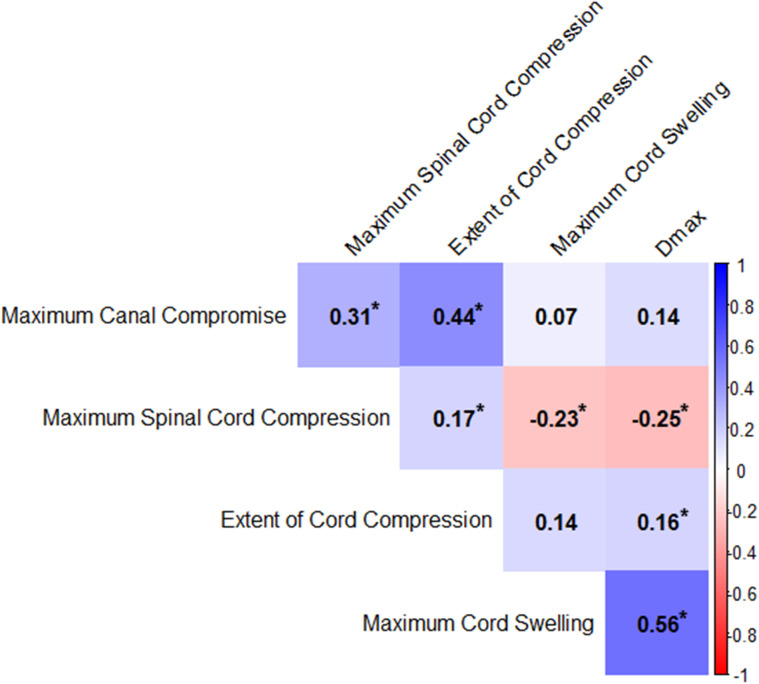
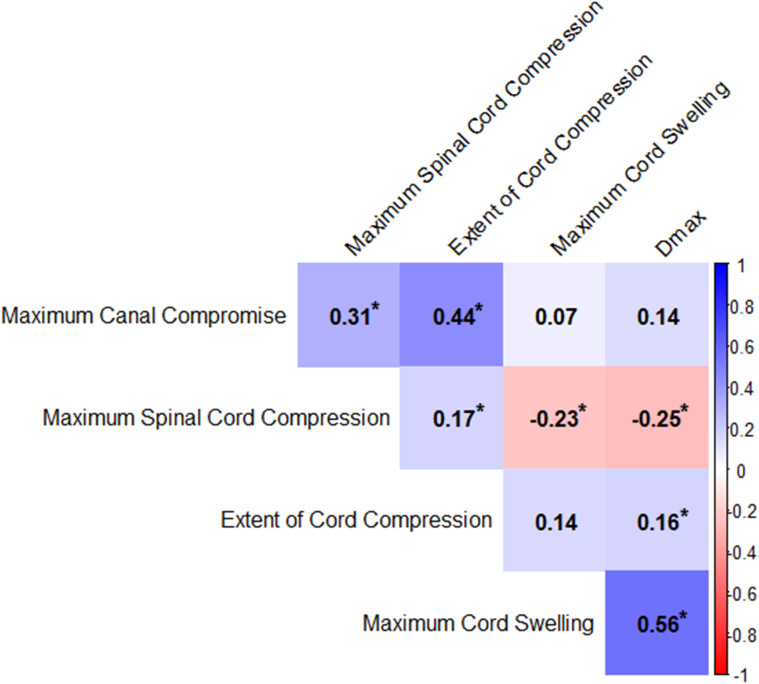
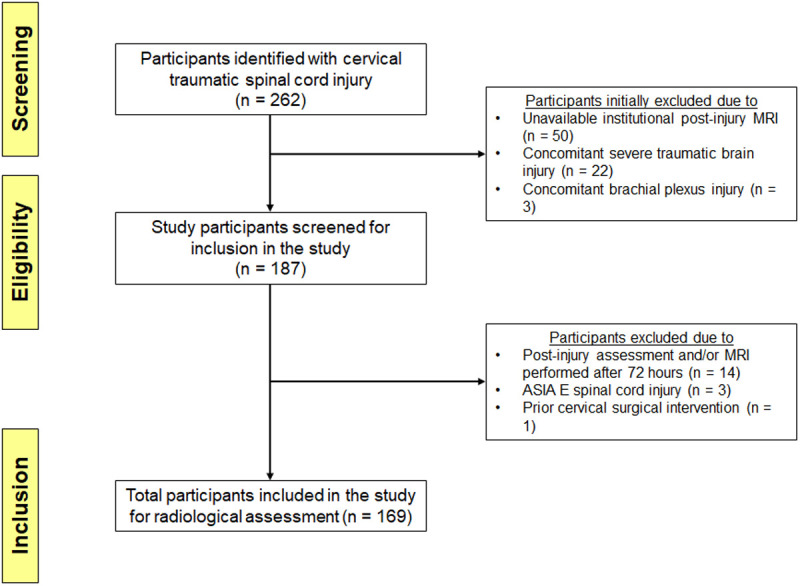
Intradural spinal cord compression impairs perfusion pressure and is putatively rate-limiting for recovery after traumatic spinal cord injury (tSCI). After cervical tSCI, even minimally improved tissue preservation may help promote neurological recovery. To assess the nature and extent of spinal cord swelling and compression post-acute cervical tSCI, we evaluated several baseline MRI parameters including BASIC score, intramedullary lesion (IML) length, maximal canal compromise (MCC), maximal spinal cord compression (MSCC), extent of cord compression (ECC), maximal swollen anteroposterior diameter adjacent to injury site (Dmax), and maximal cord swelling (MCS) in 169 consecutive patients across 2 centers. In patients with either primarily intradural or combined (MSCC ≤5% or >5%, respectively) cord compression, we examined the predictive value of clinical and imaging admission parameters on American Spinal Injury Association Impairment Scale (AIS) severity and conversion up to 1-year follow-up. 37 (21.9%) patients presented with primarily intradural while 132 (78.1%) had combined cord compression. MSCC, MCS, and Dmax values differed significantly between the two groups (p < 0.0001, < 0.01 and < 0.001, respectively). MSCC was associated with age, MCC and MCS at baseline, while MCS was associated with age, MSCC and Dmax, on multivariable analysis. Logistic regression analysis of areas under receiver operating characteristic curve (AUROC) confirmed ECC (AUC 0.678) and MCS (AUC 0.922) as good and excellent predictors, respectively of AIS-conversion at 1-year for intradural compression participants. Additionally, MCS was significantly more accurate in predicting AIS-conversion in intradural group and the probability of AIS-conversion significantly decreased with each 1% increase in MCS (p = 0.003; OR 0.949), for both compression subtypes. In conclusion, baseline measures of cord swelling predict AIS-conversion likelihood up to 1-year. The deleterious effects of intradural cord compression, either isolated or presenting with extradural compression, may benefit from supplemental decompression strategies in addition to current standard-of-care.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


