Ankita Nekkanti, Harishankar Gopakumar, Muhammad Asghar, Manasa Kandula, Srinivas Puli
{"title":"超声内镜引导下肝积液引流:来自一个病例系列的见解。","authors":"Ankita Nekkanti, Harishankar Gopakumar, Muhammad Asghar, Manasa Kandula, Srinivas Puli","doi":"10.1159/000546485","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hepatic cysts, commonly discovered incidentally, can become symptomatic due to complications like infection, rupture, or mass effect. Traditional management options include percutaneous drainage, open surgical or laparoscopic deroofing, and liver resection. We present a case series of 3 patients with complex fluid collections in the liver managed by endoscopic ultrasound (EUS)-guided drainage using lumen-apposing metal stent (LAMS) placement. While reports exist from other countries, our study contributes a series of cases from the USA.</p><p><strong>Case presentation: </strong>Three patients, average age 75 years (two men, one woman), underwent EUS-guided drainage using LAMS for an infected liver cyst, infected liver hematoma within a hepatocellular carcinoma lesion, and a symptomatic simple liver cyst, respectively. All the hepatic fluid collections were in the left hepatic lobe and had an average diameter of 11 centimeters (cm). Only the female patient with a symptomatic cyst had prior percutaneous drainage. Successful LAMS placement was achieved in all cases. Clinical success, defined as cyst resolution or significant size reduction, was observed in all patients. The superinfected liver cyst showed complete resolution, yet the stent remained in place as the patient transitioned to hospice and subsequently passed away. In the case of the superinfected liver hematoma, the stent was removed after 2 months. No recurrence was observed in follow-up imaging 8 months later, and the patient passed away. The symptomatic simple liver cyst patient had the stent removed 15 months later, with no recurrence in imaging 11 months of post-stent removal.</p><p><strong>Conclusion: </strong>EUS-guided LAMS placement emerges as a less invasive and viable option for treating symptomatic and/or infected hepatic fluid collections compared to surgery or percutaneous drainage. While it may be a preferable choice in institutions with the requisite expertise, further studies are essential to establish its definitive role as a first-line intervention.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"548-555"},"PeriodicalIF":0.6000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331227/pdf/","citationCount":"0","resultStr":"{\"title\":\"Endoscopic Ultrasound-Guided Drainage of Hepatic Fluid Collections: Insights from a Case Series.\",\"authors\":\"Ankita Nekkanti, Harishankar Gopakumar, Muhammad Asghar, Manasa Kandula, Srinivas Puli\",\"doi\":\"10.1159/000546485\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hepatic cysts, commonly discovered incidentally, can become symptomatic due to complications like infection, rupture, or mass effect. Traditional management options include percutaneous drainage, open surgical or laparoscopic deroofing, and liver resection. We present a case series of 3 patients with complex fluid collections in the liver managed by endoscopic ultrasound (EUS)-guided drainage using lumen-apposing metal stent (LAMS) placement. While reports exist from other countries, our study contributes a series of cases from the USA.</p><p><strong>Case presentation: </strong>Three patients, average age 75 years (two men, one woman), underwent EUS-guided drainage using LAMS for an infected liver cyst, infected liver hematoma within a hepatocellular carcinoma lesion, and a symptomatic simple liver cyst, respectively. All the hepatic fluid collections were in the left hepatic lobe and had an average diameter of 11 centimeters (cm). Only the female patient with a symptomatic cyst had prior percutaneous drainage. Successful LAMS placement was achieved in all cases. Clinical success, defined as cyst resolution or significant size reduction, was observed in all patients. The superinfected liver cyst showed complete resolution, yet the stent remained in place as the patient transitioned to hospice and subsequently passed away. In the case of the superinfected liver hematoma, the stent was removed after 2 months. No recurrence was observed in follow-up imaging 8 months later, and the patient passed away. The symptomatic simple liver cyst patient had the stent removed 15 months later, with no recurrence in imaging 11 months of post-stent removal.</p><p><strong>Conclusion: </strong>EUS-guided LAMS placement emerges as a less invasive and viable option for treating symptomatic and/or infected hepatic fluid collections compared to surgery or percutaneous drainage. While it may be a preferable choice in institutions with the requisite expertise, further studies are essential to establish its definitive role as a first-line intervention.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"19 1\",\"pages\":\"548-555\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331227/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000546485\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546485","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Endoscopic Ultrasound-Guided Drainage of Hepatic Fluid Collections: Insights from a Case Series.
Introduction: Hepatic cysts, commonly discovered incidentally, can become symptomatic due to complications like infection, rupture, or mass effect. Traditional management options include percutaneous drainage, open surgical or laparoscopic deroofing, and liver resection. We present a case series of 3 patients with complex fluid collections in the liver managed by endoscopic ultrasound (EUS)-guided drainage using lumen-apposing metal stent (LAMS) placement. While reports exist from other countries, our study contributes a series of cases from the USA.
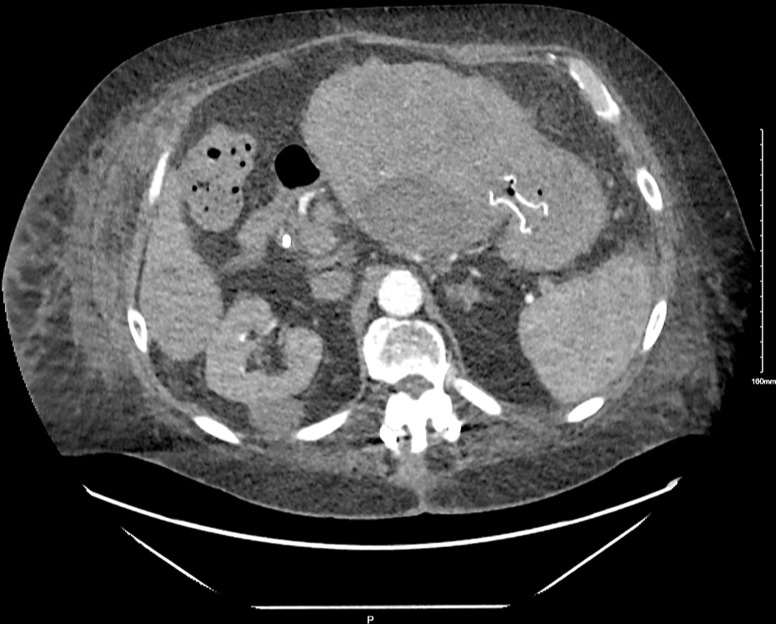
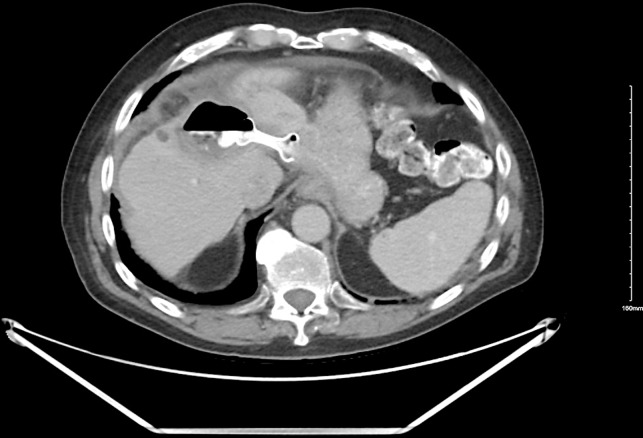
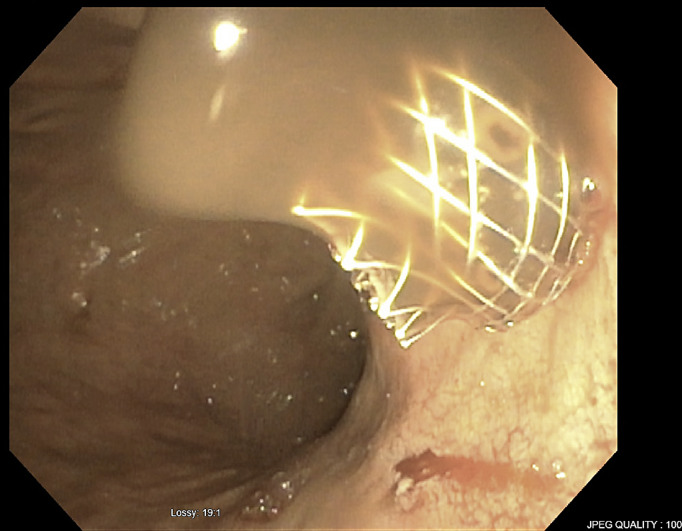
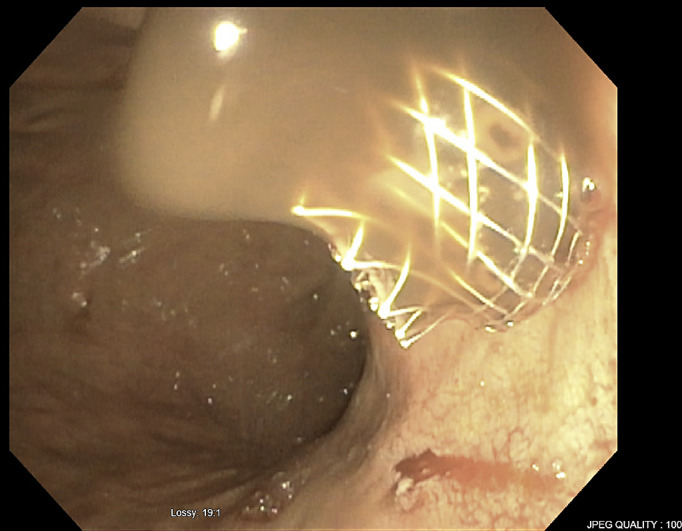
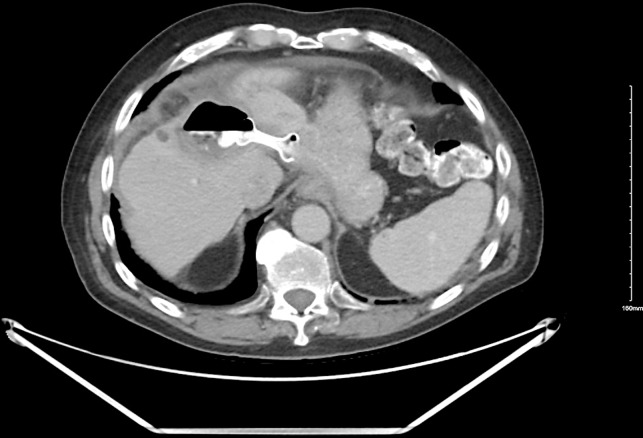
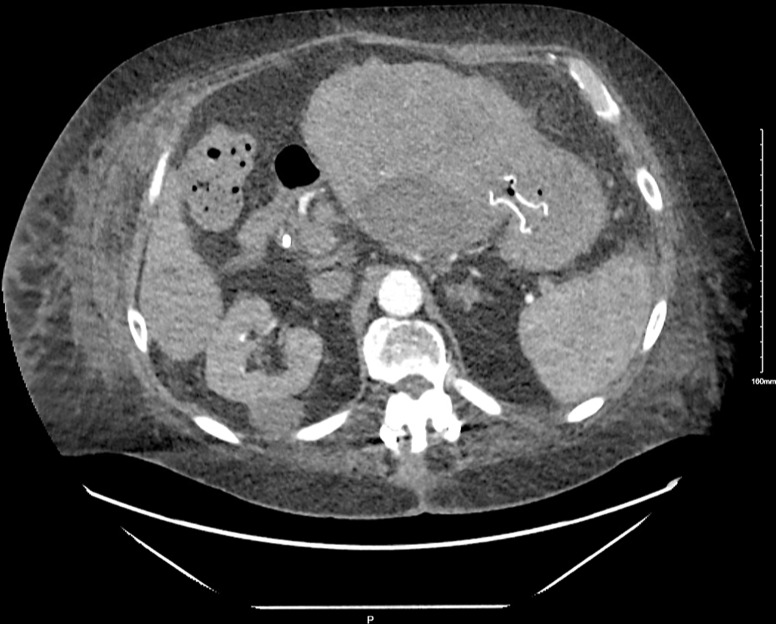
Case presentation: Three patients, average age 75 years (two men, one woman), underwent EUS-guided drainage using LAMS for an infected liver cyst, infected liver hematoma within a hepatocellular carcinoma lesion, and a symptomatic simple liver cyst, respectively. All the hepatic fluid collections were in the left hepatic lobe and had an average diameter of 11 centimeters (cm). Only the female patient with a symptomatic cyst had prior percutaneous drainage. Successful LAMS placement was achieved in all cases. Clinical success, defined as cyst resolution or significant size reduction, was observed in all patients. The superinfected liver cyst showed complete resolution, yet the stent remained in place as the patient transitioned to hospice and subsequently passed away. In the case of the superinfected liver hematoma, the stent was removed after 2 months. No recurrence was observed in follow-up imaging 8 months later, and the patient passed away. The symptomatic simple liver cyst patient had the stent removed 15 months later, with no recurrence in imaging 11 months of post-stent removal.
Conclusion: EUS-guided LAMS placement emerges as a less invasive and viable option for treating symptomatic and/or infected hepatic fluid collections compared to surgery or percutaneous drainage. While it may be a preferable choice in institutions with the requisite expertise, further studies are essential to establish its definitive role as a first-line intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


