Qin Xu, Luyu Li, Bo Li, Zouying Tang, Yaxian Ma, Limei Tao, Rui Ma, Li Zhuan
{"title":"多模式治疗合并阿什曼综合征、复发性妊娠丢失和多囊卵巢综合征患者的活产:1例报告和文献回顾。","authors":"Qin Xu, Luyu Li, Bo Li, Zouying Tang, Yaxian Ma, Limei Tao, Rui Ma, Li Zhuan","doi":"10.1186/s40834-025-00384-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Improving the endometrial thickness (EMT) and pregnancy outcomes in cases of thin endometrium (TE) induced by severe intrauterine adhesion (IUA) is a significant clinical challenge. This report provides insight into a potential protocol for improving EMT and pregnancy outcomes in challenging cases of TE induced by IUA, especially for patients with concurrent polycystic ovary syndrome (PCOS) and experiencing recurrent spontaneous abortion (RSA).</p><p><strong>Case presentation: </strong>We report the case of a 29-year-old woman with severe IUA, RSA, and PCOS, who experienced three spontaneous abortions. Copy number variations (CNV's) detection of fetal villi from the last abortion indicated Turner syndrome. Hysteroscopic adhesiolysis (HA) had been performed twice previously. She subsequently underwent superovulation using an antagonist regimen, resulting in oocyte retrieval and cryopreservation of four transplantable blastocysts after genetic testing. After three rounds of HA, the uterine cavity shape returned to normal. She then received two cycles of Femoston and/or estradiol valerate therapy combined with oral low-dose aspirin, vaginal sildenafil, pelvic floor electrical stimulation, and uterine perfusion platelet-rich plasma (PRP); however, the frozen embryo transfer (FET) was canceled as the EMT remained 4.9 mm and 3.9 mm. After three additional HA procedures and one hysteroscopy, the uterine cavity returned to normal. She then received tamoxifen (TAM) with estradiol valerate and human menopausal gonadotropin (HMG), achieving an EMT of 7.5 mm after ovulation. Ultimately, the frozen transfer of a 4BB blastocyst resulted in the birth of a healthy baby boy.</p><p><strong>Conclusions: </strong>This case highlights the complexities of managing TE induced by IUA using HA and assisted reproductive techniques. It also suggests that patients with TE complicated by PCOS and RSA can be treated with TAM, followed by estradiol valerate and HMG, to improve the EMT and pregnancy outcomes of FET.</p>","PeriodicalId":93956,"journal":{"name":"Contraception and reproductive medicine","volume":"10 1","pages":"45"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330053/pdf/","citationCount":"0","resultStr":"{\"title\":\"Live birth following multimodal therapy in a patient with asherman's syndrome, recurrent pregnancy loss, and polycystic ovarian syndrome: a case report and literature review.\",\"authors\":\"Qin Xu, Luyu Li, Bo Li, Zouying Tang, Yaxian Ma, Limei Tao, Rui Ma, Li Zhuan\",\"doi\":\"10.1186/s40834-025-00384-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Improving the endometrial thickness (EMT) and pregnancy outcomes in cases of thin endometrium (TE) induced by severe intrauterine adhesion (IUA) is a significant clinical challenge. This report provides insight into a potential protocol for improving EMT and pregnancy outcomes in challenging cases of TE induced by IUA, especially for patients with concurrent polycystic ovary syndrome (PCOS) and experiencing recurrent spontaneous abortion (RSA).</p><p><strong>Case presentation: </strong>We report the case of a 29-year-old woman with severe IUA, RSA, and PCOS, who experienced three spontaneous abortions. Copy number variations (CNV's) detection of fetal villi from the last abortion indicated Turner syndrome. Hysteroscopic adhesiolysis (HA) had been performed twice previously. She subsequently underwent superovulation using an antagonist regimen, resulting in oocyte retrieval and cryopreservation of four transplantable blastocysts after genetic testing. After three rounds of HA, the uterine cavity shape returned to normal. She then received two cycles of Femoston and/or estradiol valerate therapy combined with oral low-dose aspirin, vaginal sildenafil, pelvic floor electrical stimulation, and uterine perfusion platelet-rich plasma (PRP); however, the frozen embryo transfer (FET) was canceled as the EMT remained 4.9 mm and 3.9 mm. After three additional HA procedures and one hysteroscopy, the uterine cavity returned to normal. She then received tamoxifen (TAM) with estradiol valerate and human menopausal gonadotropin (HMG), achieving an EMT of 7.5 mm after ovulation. Ultimately, the frozen transfer of a 4BB blastocyst resulted in the birth of a healthy baby boy.</p><p><strong>Conclusions: </strong>This case highlights the complexities of managing TE induced by IUA using HA and assisted reproductive techniques. It also suggests that patients with TE complicated by PCOS and RSA can be treated with TAM, followed by estradiol valerate and HMG, to improve the EMT and pregnancy outcomes of FET.</p>\",\"PeriodicalId\":93956,\"journal\":{\"name\":\"Contraception and reproductive medicine\",\"volume\":\"10 1\",\"pages\":\"45\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330053/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception and reproductive medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40834-025-00384-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception and reproductive medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40834-025-00384-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Live birth following multimodal therapy in a patient with asherman's syndrome, recurrent pregnancy loss, and polycystic ovarian syndrome: a case report and literature review.
Background: Improving the endometrial thickness (EMT) and pregnancy outcomes in cases of thin endometrium (TE) induced by severe intrauterine adhesion (IUA) is a significant clinical challenge. This report provides insight into a potential protocol for improving EMT and pregnancy outcomes in challenging cases of TE induced by IUA, especially for patients with concurrent polycystic ovary syndrome (PCOS) and experiencing recurrent spontaneous abortion (RSA).
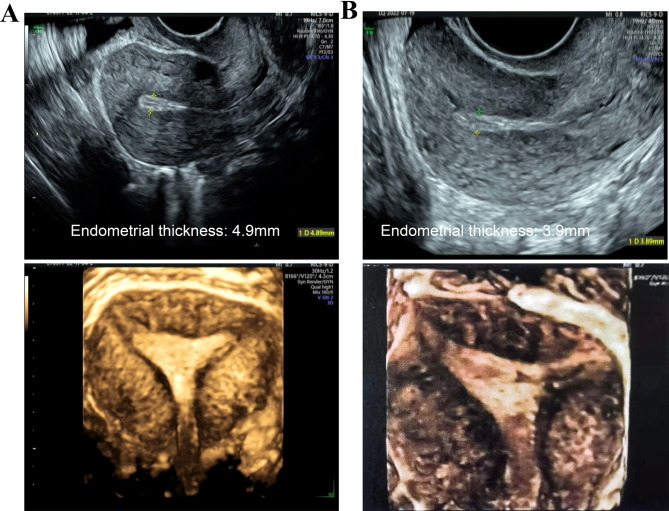
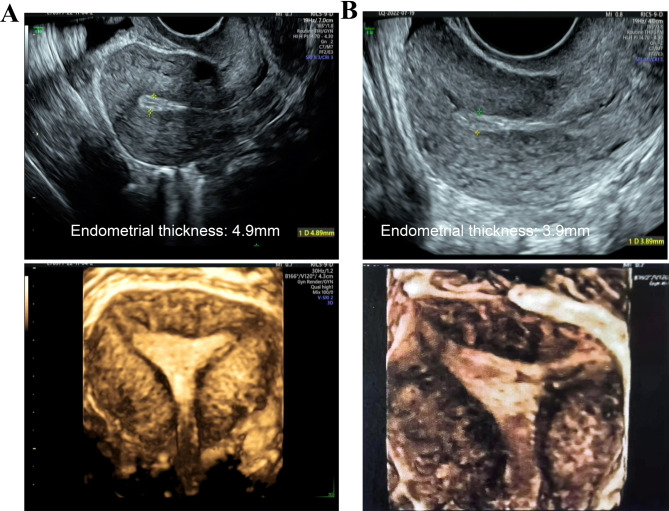
Case presentation: We report the case of a 29-year-old woman with severe IUA, RSA, and PCOS, who experienced three spontaneous abortions. Copy number variations (CNV's) detection of fetal villi from the last abortion indicated Turner syndrome. Hysteroscopic adhesiolysis (HA) had been performed twice previously. She subsequently underwent superovulation using an antagonist regimen, resulting in oocyte retrieval and cryopreservation of four transplantable blastocysts after genetic testing. After three rounds of HA, the uterine cavity shape returned to normal. She then received two cycles of Femoston and/or estradiol valerate therapy combined with oral low-dose aspirin, vaginal sildenafil, pelvic floor electrical stimulation, and uterine perfusion platelet-rich plasma (PRP); however, the frozen embryo transfer (FET) was canceled as the EMT remained 4.9 mm and 3.9 mm. After three additional HA procedures and one hysteroscopy, the uterine cavity returned to normal. She then received tamoxifen (TAM) with estradiol valerate and human menopausal gonadotropin (HMG), achieving an EMT of 7.5 mm after ovulation. Ultimately, the frozen transfer of a 4BB blastocyst resulted in the birth of a healthy baby boy.
Conclusions: This case highlights the complexities of managing TE induced by IUA using HA and assisted reproductive techniques. It also suggests that patients with TE complicated by PCOS and RSA can be treated with TAM, followed by estradiol valerate and HMG, to improve the EMT and pregnancy outcomes of FET.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


