Daniel Moreira Costa Moura, Renner Augusto Raposo Pereira, Cristiano Faria Pisani, Tan Chen Wu, Muhieddine Omar Chokr, Carina Abigail Hardy, Sissy Lara de Melo, Francisco Carlos da Costa Darrieux, Denise Tessariol Hachul, Mauricio Ibrahim Scanavacca
{"title":"心房颤动消融期间食管温度监测:一项随机研究。","authors":"Daniel Moreira Costa Moura, Renner Augusto Raposo Pereira, Cristiano Faria Pisani, Tan Chen Wu, Muhieddine Omar Chokr, Carina Abigail Hardy, Sissy Lara de Melo, Francisco Carlos da Costa Darrieux, Denise Tessariol Hachul, Mauricio Ibrahim Scanavacca","doi":"10.36660/abc.20250056","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary vein isolation (PVI) for atrial fibrillation (AF) ablation carries a risk of esophageal thermal injury (ETI), which can lead to severe complications.</p><p><strong>Objective: </strong>To evaluate three luminal esophageal temperature (LET) monitoring strategies and assess their effectiveness in reducing the incidence of ETI.</p><p><strong>Methods: </strong>Patients with AF were randomized into three PVI groups according to the temperature monitoring strategy: no LET monitoring (Group 1), LET monitoring with a single-sensor probe (SSP) thermometer (Group 2), and LET monitoring with a multisensor probe (MSP) thermometer (Group 3). In Group 1, AF ablation was performed at a fixed power of 20 W on the left atrial posterior wall. In Groups 2 and 3, AF ablation power was titrated based on LET measurements, with a cutoff temperature of 37.5 °C. Each group included 20 patients. A two-sided p-value <0.05 was considered statistically significant. The trial was registered on ClinicalTrials.gov (#NCT03645070) and International Clinical Trials Registry Platform (#RBR-2yvgyf).</p><p><strong>Results: </strong>All patients underwent PVI and esophagogastroduodenoscopy. No ETI was observed in patients monitored with an MSP thermometer. In contrast, five patients without LET monitoring and six patients monitored with an SSP thermometer developed ETI (p=0.006). Higher temperatures were recorded with an MSP thermometer (37.9 vs. 38.45 °C, p=0.018). There were no significant differences in PVI duration or total radiofrequency application time (p=0.250 and p=0.253, respectively).</p><p><strong>Conclusions: </strong>LET monitoring with an MSP thermometer during PVI significantly reduces the incidence of ETI compared to no monitoring or SSP monitoring. Implementing advanced LET monitoring strategies may enhance patient safety without compromising procedural efficiency.</p>","PeriodicalId":93887,"journal":{"name":"Arquivos brasileiros de cardiologia","volume":"122 7","pages":"e20250056"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12266716/pdf/","citationCount":"0","resultStr":"{\"title\":\"Esophageal Temperature Monitoring during Atrial Fibrillation Ablation: A Randomized Study.\",\"authors\":\"Daniel Moreira Costa Moura, Renner Augusto Raposo Pereira, Cristiano Faria Pisani, Tan Chen Wu, Muhieddine Omar Chokr, Carina Abigail Hardy, Sissy Lara de Melo, Francisco Carlos da Costa Darrieux, Denise Tessariol Hachul, Mauricio Ibrahim Scanavacca\",\"doi\":\"10.36660/abc.20250056\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pulmonary vein isolation (PVI) for atrial fibrillation (AF) ablation carries a risk of esophageal thermal injury (ETI), which can lead to severe complications.</p><p><strong>Objective: </strong>To evaluate three luminal esophageal temperature (LET) monitoring strategies and assess their effectiveness in reducing the incidence of ETI.</p><p><strong>Methods: </strong>Patients with AF were randomized into three PVI groups according to the temperature monitoring strategy: no LET monitoring (Group 1), LET monitoring with a single-sensor probe (SSP) thermometer (Group 2), and LET monitoring with a multisensor probe (MSP) thermometer (Group 3). In Group 1, AF ablation was performed at a fixed power of 20 W on the left atrial posterior wall. In Groups 2 and 3, AF ablation power was titrated based on LET measurements, with a cutoff temperature of 37.5 °C. Each group included 20 patients. A two-sided p-value <0.05 was considered statistically significant. The trial was registered on ClinicalTrials.gov (#NCT03645070) and International Clinical Trials Registry Platform (#RBR-2yvgyf).</p><p><strong>Results: </strong>All patients underwent PVI and esophagogastroduodenoscopy. No ETI was observed in patients monitored with an MSP thermometer. In contrast, five patients without LET monitoring and six patients monitored with an SSP thermometer developed ETI (p=0.006). Higher temperatures were recorded with an MSP thermometer (37.9 vs. 38.45 °C, p=0.018). There were no significant differences in PVI duration or total radiofrequency application time (p=0.250 and p=0.253, respectively).</p><p><strong>Conclusions: </strong>LET monitoring with an MSP thermometer during PVI significantly reduces the incidence of ETI compared to no monitoring or SSP monitoring. Implementing advanced LET monitoring strategies may enhance patient safety without compromising procedural efficiency.</p>\",\"PeriodicalId\":93887,\"journal\":{\"name\":\"Arquivos brasileiros de cardiologia\",\"volume\":\"122 7\",\"pages\":\"e20250056\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12266716/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arquivos brasileiros de cardiologia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36660/abc.20250056\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cardiologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36660/abc.20250056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:肺静脉隔离(PVI)治疗心房颤动(AF)消融具有食管热损伤(ETI)的风险,可导致严重的并发症。目的:评价三种腔内食管温度(LET)监测策略对降低ETI发生率的效果。方法:根据温度监测策略,将房颤患者随机分为3组:无LET监测组(1组)、单传感器探针(SSP)体温计LET监测组(2组)和多传感器探针(MSP)体温计LET监测组(3组)。组1左房后壁以固定功率20w进行房颤消融。在第2组和第3组中,根据LET测量值滴定AF消融功率,截止温度为37.5℃。每组20例。双侧p值结果:所有患者均行PVI和食管胃十二指肠镜检查。使用MSP体温计监测的患者未观察到ETI。相比之下,5名未进行LET监测的患者和6名使用SSP体温计监测的患者发生了ETI (p=0.006)。用MSP温度计记录较高的温度(37.9°C vs. 38.45°C, p=0.018)。PVI持续时间和总射频应用时间无显著差异(p=0.250和p=0.253)。结论:与不监测或SSP监测相比,PVI期间使用MSP体温计监测LET可显著降低ETI的发生率。实施先进的LET监测策略可以在不影响程序效率的情况下提高患者安全。
Esophageal Temperature Monitoring during Atrial Fibrillation Ablation: A Randomized Study.
Background: Pulmonary vein isolation (PVI) for atrial fibrillation (AF) ablation carries a risk of esophageal thermal injury (ETI), which can lead to severe complications.
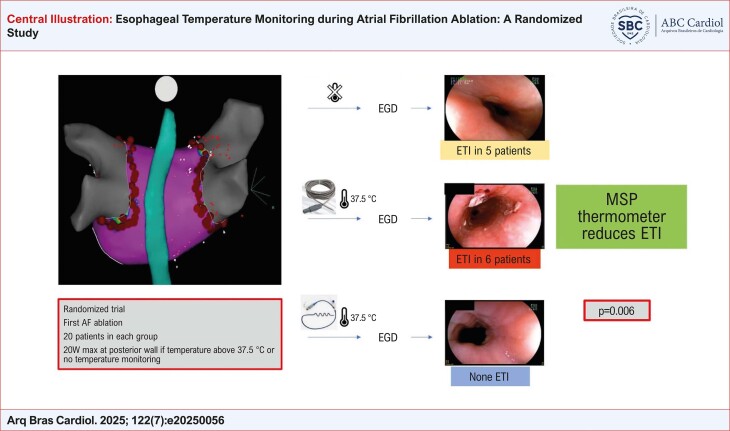
Objective: To evaluate three luminal esophageal temperature (LET) monitoring strategies and assess their effectiveness in reducing the incidence of ETI.
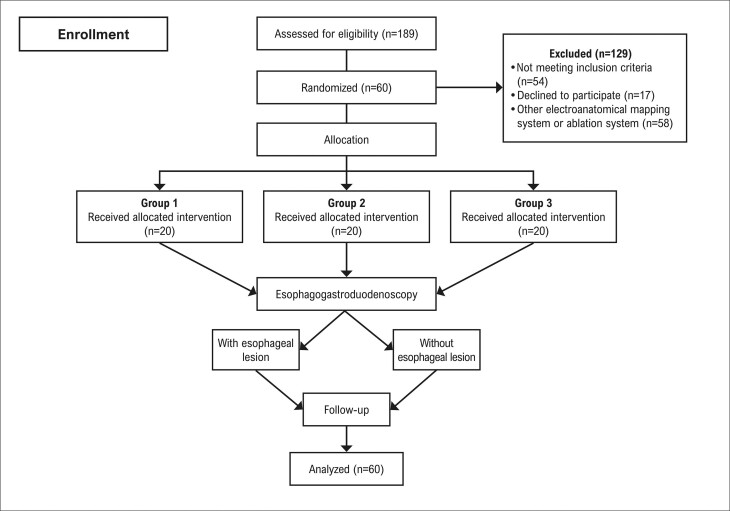
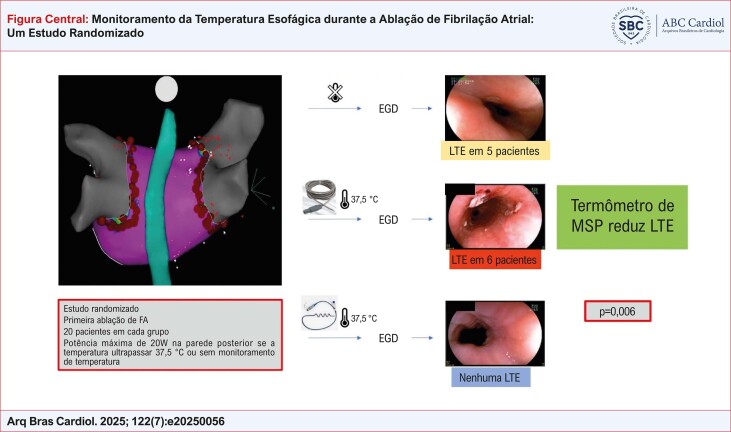
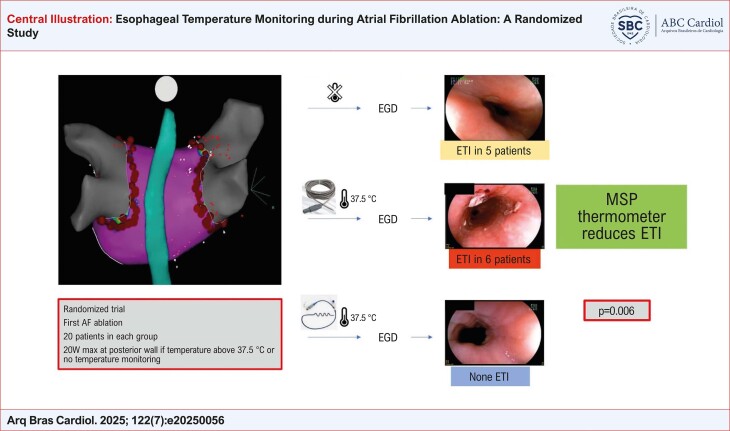
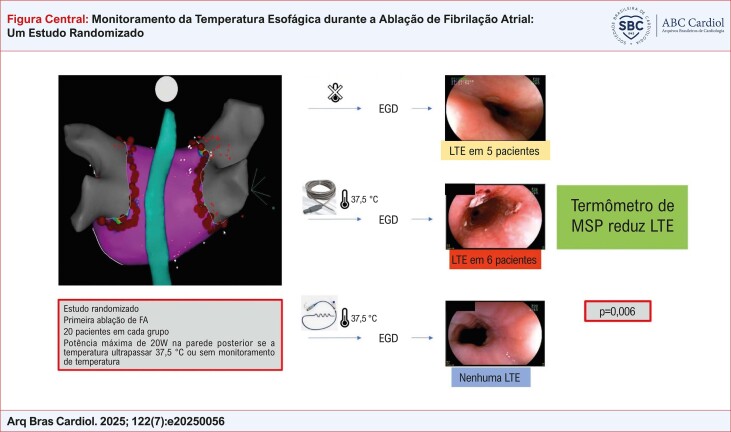
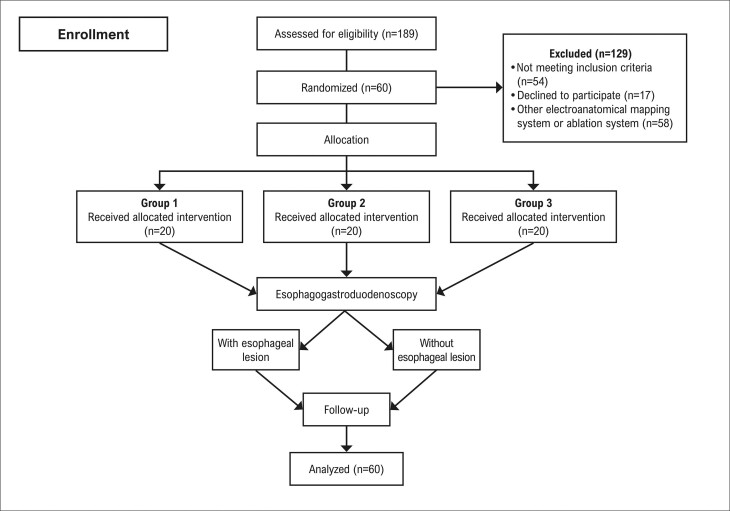
Methods: Patients with AF were randomized into three PVI groups according to the temperature monitoring strategy: no LET monitoring (Group 1), LET monitoring with a single-sensor probe (SSP) thermometer (Group 2), and LET monitoring with a multisensor probe (MSP) thermometer (Group 3). In Group 1, AF ablation was performed at a fixed power of 20 W on the left atrial posterior wall. In Groups 2 and 3, AF ablation power was titrated based on LET measurements, with a cutoff temperature of 37.5 °C. Each group included 20 patients. A two-sided p-value <0.05 was considered statistically significant. The trial was registered on ClinicalTrials.gov (#NCT03645070) and International Clinical Trials Registry Platform (#RBR-2yvgyf).
Results: All patients underwent PVI and esophagogastroduodenoscopy. No ETI was observed in patients monitored with an MSP thermometer. In contrast, five patients without LET monitoring and six patients monitored with an SSP thermometer developed ETI (p=0.006). Higher temperatures were recorded with an MSP thermometer (37.9 vs. 38.45 °C, p=0.018). There were no significant differences in PVI duration or total radiofrequency application time (p=0.250 and p=0.253, respectively).
Conclusions: LET monitoring with an MSP thermometer during PVI significantly reduces the incidence of ETI compared to no monitoring or SSP monitoring. Implementing advanced LET monitoring strategies may enhance patient safety without compromising procedural efficiency.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


