{"title":"紧急脾栓塞治疗难治性免疫性血小板减少症合并重症出血1例。","authors":"Hayabusa Takano, Naoki Hara, Eri Nakajima, Kouhei Katsuda, Kenki Usami, Ayaka Hasegawa, Jun Matsuda, Satoshi Arino, Nobuo Sasaki, Naoki Kojima, Hiroshi Inagawa, Yasusei Okada, Akira Fujita","doi":"10.21037/acr-25-25","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune thrombocytopenia (ITP) is characterized by decreased platelet count due to immunological mechanisms. First-line treatment is corticosteroids, with thrombopoietin receptor agonists, rituximab, and splenectomy as second-line options. While surgical splenectomy is effective, it poses high bleeding risks in severe thrombocytopenia. Splenic embolization (SE) is considered an alternative to splenectomy for the treatment of steroid-refractory chronic ITP and has been reported to be an effective and minimally invasive option. However, there are few reports of SE being performed for acute ITP with life-threatening bleeding.</p><p><strong>Case description: </strong>A 63-year-old man presented in shock with oral bleeding, bloody stools, and recurrent syncope. Laboratory tests revealed severe thrombocytopenia (4,000/mm<sup>3</sup> platelets) and elevated platelet-associated immunoglobulin G (PA-IgG), leading to ITP diagnosis. Despite platelet transfusions, intravenous immunoglobulin, and high-dose steroids, his condition worsened with alveolar hemorrhage developing on day 3. Given the surgical risks, emergency SE was performed on day 5 using coils and gelatin sponge. Following SE and thrombopoietin receptor agonist administration, platelet counts improved from day 6, allowing discontinuation of transfusions by day 11. The patient was discharged from the intensive care unit on day 12 with stabilized platelets and improved respiratory status.</p><p><strong>Conclusions: </strong>This case demonstrates that emergency SE can be an effective and safe alternative to splenectomy for refractory ITP with life-threatening bleeding, particularly when severe thrombocytopenia precludes surgical intervention. The rapid improvement in platelet counts suggests SE could be a viable emergency treatment option.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"105"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319611/pdf/","citationCount":"0","resultStr":"{\"title\":\"Emergent splenic embolization for refractory immune thrombocytopenia with critical bleeding: a case report.\",\"authors\":\"Hayabusa Takano, Naoki Hara, Eri Nakajima, Kouhei Katsuda, Kenki Usami, Ayaka Hasegawa, Jun Matsuda, Satoshi Arino, Nobuo Sasaki, Naoki Kojima, Hiroshi Inagawa, Yasusei Okada, Akira Fujita\",\"doi\":\"10.21037/acr-25-25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Immune thrombocytopenia (ITP) is characterized by decreased platelet count due to immunological mechanisms. First-line treatment is corticosteroids, with thrombopoietin receptor agonists, rituximab, and splenectomy as second-line options. While surgical splenectomy is effective, it poses high bleeding risks in severe thrombocytopenia. Splenic embolization (SE) is considered an alternative to splenectomy for the treatment of steroid-refractory chronic ITP and has been reported to be an effective and minimally invasive option. However, there are few reports of SE being performed for acute ITP with life-threatening bleeding.</p><p><strong>Case description: </strong>A 63-year-old man presented in shock with oral bleeding, bloody stools, and recurrent syncope. Laboratory tests revealed severe thrombocytopenia (4,000/mm<sup>3</sup> platelets) and elevated platelet-associated immunoglobulin G (PA-IgG), leading to ITP diagnosis. Despite platelet transfusions, intravenous immunoglobulin, and high-dose steroids, his condition worsened with alveolar hemorrhage developing on day 3. Given the surgical risks, emergency SE was performed on day 5 using coils and gelatin sponge. Following SE and thrombopoietin receptor agonist administration, platelet counts improved from day 6, allowing discontinuation of transfusions by day 11. The patient was discharged from the intensive care unit on day 12 with stabilized platelets and improved respiratory status.</p><p><strong>Conclusions: </strong>This case demonstrates that emergency SE can be an effective and safe alternative to splenectomy for refractory ITP with life-threatening bleeding, particularly when severe thrombocytopenia precludes surgical intervention. The rapid improvement in platelet counts suggests SE could be a viable emergency treatment option.</p>\",\"PeriodicalId\":29752,\"journal\":{\"name\":\"AME Case Reports\",\"volume\":\"9 \",\"pages\":\"105\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319611/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AME Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/acr-25-25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-25-25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Emergent splenic embolization for refractory immune thrombocytopenia with critical bleeding: a case report.
Background: Immune thrombocytopenia (ITP) is characterized by decreased platelet count due to immunological mechanisms. First-line treatment is corticosteroids, with thrombopoietin receptor agonists, rituximab, and splenectomy as second-line options. While surgical splenectomy is effective, it poses high bleeding risks in severe thrombocytopenia. Splenic embolization (SE) is considered an alternative to splenectomy for the treatment of steroid-refractory chronic ITP and has been reported to be an effective and minimally invasive option. However, there are few reports of SE being performed for acute ITP with life-threatening bleeding.
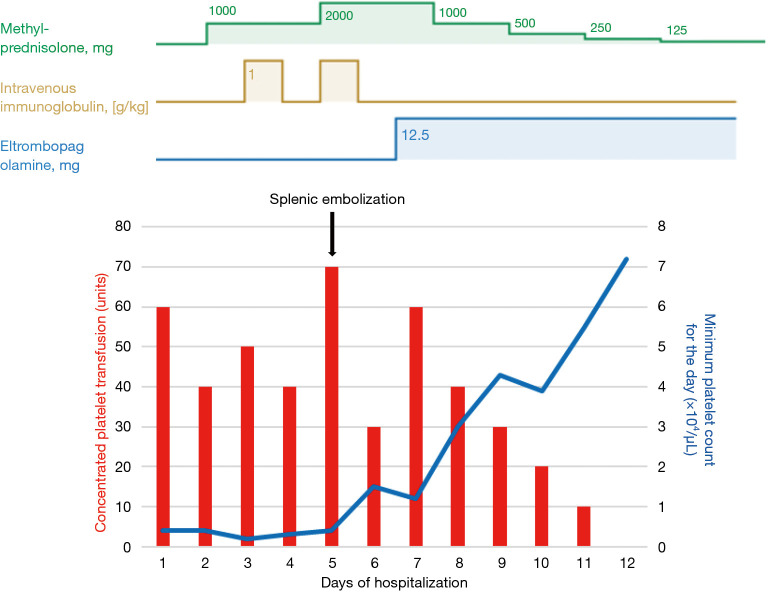
Case description: A 63-year-old man presented in shock with oral bleeding, bloody stools, and recurrent syncope. Laboratory tests revealed severe thrombocytopenia (4,000/mm3 platelets) and elevated platelet-associated immunoglobulin G (PA-IgG), leading to ITP diagnosis. Despite platelet transfusions, intravenous immunoglobulin, and high-dose steroids, his condition worsened with alveolar hemorrhage developing on day 3. Given the surgical risks, emergency SE was performed on day 5 using coils and gelatin sponge. Following SE and thrombopoietin receptor agonist administration, platelet counts improved from day 6, allowing discontinuation of transfusions by day 11. The patient was discharged from the intensive care unit on day 12 with stabilized platelets and improved respiratory status.
Conclusions: This case demonstrates that emergency SE can be an effective and safe alternative to splenectomy for refractory ITP with life-threatening bleeding, particularly when severe thrombocytopenia precludes surgical intervention. The rapid improvement in platelet counts suggests SE could be a viable emergency treatment option.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


