Roberta Scarmignan, Gaetano Alfano, Niccolò Morisi, Francesco Fontana, Giacomo Mori, Marco Ferrarini, Camilla Ferri, Laura Tonelli, Giulia Ligabue, Riccardo Magistroni, Mariacristina Gregorini, Gabriele Donati
{"title":"腹膜透析患者的长期死亡率和技术生存率:单中心25年回顾性分析。","authors":"Roberta Scarmignan, Gaetano Alfano, Niccolò Morisi, Francesco Fontana, Giacomo Mori, Marco Ferrarini, Camilla Ferri, Laura Tonelli, Giulia Ligabue, Riccardo Magistroni, Mariacristina Gregorini, Gabriele Donati","doi":"10.1093/ckj/sfaf215","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We comprehensively assessed patient survival and the duration of peritoneal dialysis (PD) treatment over a 25-year period within our PD unit.</p><p><strong>Methods: </strong>We retrospectively evaluated 497 PD patients who initiated PD between 1996 and 2021. The cohort was divided into three distinct periods based on pivotal events, such as the introduction of more biocompatible dialysis solutions and the initiation of remote monitoring technologies. Kaplan-Meier survival assessments, Cox proportional hazards model and Gray subdistribution hazard model were employed to evaluate patient survival and PD-to-hemodialysis (HD) transfer.</p><p><strong>Results: </strong>The use of PD as the initial treatment increased significantly over the years. Mean age was 63.5 ± 15.7 years; 61% were male, and 61% had three or more comorbidities including hypertension (81%), dyslipidemia (66%), cardiovascular disease (56%) and diabetes (16%). The five-year mortality rate was 40%. Risk factors for mortality included continuous ambulatory peritoneal dialysis (CAPD) [hazard ratio (HR) = 2.63, 95% confidence interval (CI) 1.76-3.93; <i>P</i> < .001], older age (HR = 2.96, 95% CI 1.98-4.43; <i>P</i> < .001), cardiovascular disease (HR = 1.96, 95% CI 1.31-2.95; <i>P</i> = .001) and the use of renin-angiotensin-aldosterone system inhibitors (RAASi) (HR = 1.81, 95% CI 1.22-2.70; <i>P</i> = .004). At 5 years, 48% of patients remained on PD. In the Cox model, risk factors for PD-to-HD transfer included CAPD (HR = 1.62, 95% CI 1.21-2.16; <i>P</i> = .001). RAASi use (HR = 0.66, 95% CI 0.46-0.94; <i>P</i> = .02) and female sex (HR = 0.70, 95% CI 0.51-0.96; <i>P</i> = .03) were associated with longer PD duration.</p><p><strong>Conclusions: </strong>The study provides insights into the changing landscape of PD. Advances in PD solutions and remote monitoring have contributed to changes in PD outcomes and its increased adoption over the years. Given the observational nature of the study, caution is warranted in interpreting the association of both CAPD and RAASi with mortality.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 8","pages":"sfaf215"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319534/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term mortality and technique survival in peritoneal dialysis patients: a 25-year retrospective analysis in a single center.\",\"authors\":\"Roberta Scarmignan, Gaetano Alfano, Niccolò Morisi, Francesco Fontana, Giacomo Mori, Marco Ferrarini, Camilla Ferri, Laura Tonelli, Giulia Ligabue, Riccardo Magistroni, Mariacristina Gregorini, Gabriele Donati\",\"doi\":\"10.1093/ckj/sfaf215\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We comprehensively assessed patient survival and the duration of peritoneal dialysis (PD) treatment over a 25-year period within our PD unit.</p><p><strong>Methods: </strong>We retrospectively evaluated 497 PD patients who initiated PD between 1996 and 2021. The cohort was divided into three distinct periods based on pivotal events, such as the introduction of more biocompatible dialysis solutions and the initiation of remote monitoring technologies. Kaplan-Meier survival assessments, Cox proportional hazards model and Gray subdistribution hazard model were employed to evaluate patient survival and PD-to-hemodialysis (HD) transfer.</p><p><strong>Results: </strong>The use of PD as the initial treatment increased significantly over the years. Mean age was 63.5 ± 15.7 years; 61% were male, and 61% had three or more comorbidities including hypertension (81%), dyslipidemia (66%), cardiovascular disease (56%) and diabetes (16%). The five-year mortality rate was 40%. Risk factors for mortality included continuous ambulatory peritoneal dialysis (CAPD) [hazard ratio (HR) = 2.63, 95% confidence interval (CI) 1.76-3.93; <i>P</i> < .001], older age (HR = 2.96, 95% CI 1.98-4.43; <i>P</i> < .001), cardiovascular disease (HR = 1.96, 95% CI 1.31-2.95; <i>P</i> = .001) and the use of renin-angiotensin-aldosterone system inhibitors (RAASi) (HR = 1.81, 95% CI 1.22-2.70; <i>P</i> = .004). At 5 years, 48% of patients remained on PD. In the Cox model, risk factors for PD-to-HD transfer included CAPD (HR = 1.62, 95% CI 1.21-2.16; <i>P</i> = .001). RAASi use (HR = 0.66, 95% CI 0.46-0.94; <i>P</i> = .02) and female sex (HR = 0.70, 95% CI 0.51-0.96; <i>P</i> = .03) were associated with longer PD duration.</p><p><strong>Conclusions: </strong>The study provides insights into the changing landscape of PD. Advances in PD solutions and remote monitoring have contributed to changes in PD outcomes and its increased adoption over the years. Given the observational nature of the study, caution is warranted in interpreting the association of both CAPD and RAASi with mortality.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 8\",\"pages\":\"sfaf215\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-07-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319534/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf215\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf215","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:我们全面评估了25年来腹膜透析(PD)治疗患者的生存和持续时间。方法:我们回顾性评估了1996年至2021年间497例PD患者。该队列根据关键事件分为三个不同的时期,例如引入更多生物相容性透析溶液和启动远程监测技术。采用Kaplan-Meier生存评估、Cox比例风险模型和Gray亚分布风险模型评估患者生存和pd -to- blood dialysis (HD)转移。结果:多年来,PD作为初始治疗的使用显著增加。平均年龄63.5±15.7岁;61%为男性,61%有三种或三种以上合并症,包括高血压(81%)、血脂异常(66%)、心血管疾病(56%)和糖尿病(16%)。5年死亡率为40%。死亡的危险因素包括:连续非卧床腹膜透析(CAPD)[危险比(HR) = 2.63, 95%可信区间(CI) 1.76-3.93;P P = .001)和肾素-血管紧张素-醛固酮系统抑制剂(RAASi)的使用(HR = 1.81, 95% CI 1.22-2.70;p = .004)。5年后,48%的患者继续接受PD治疗。在Cox模型中,PD-to-HD转移的危险因素包括CAPD (HR = 1.62, 95% CI 1.21-2.16;p = .001)。RAASi使用(HR = 0.66, 95% CI 0.46-0.94;P = 0.02)和女性(HR = 0.70, 95% CI 0.51-0.96;P = .03)与较长的PD持续时间相关。结论:该研究为PD的变化提供了见解。多年来,PD解决方案和远程监控的进步促进了PD结果的变化和其采用率的增加。鉴于该研究的观察性质,在解释CAPD和RAASi与死亡率的关系时需要谨慎。
Long-term mortality and technique survival in peritoneal dialysis patients: a 25-year retrospective analysis in a single center.
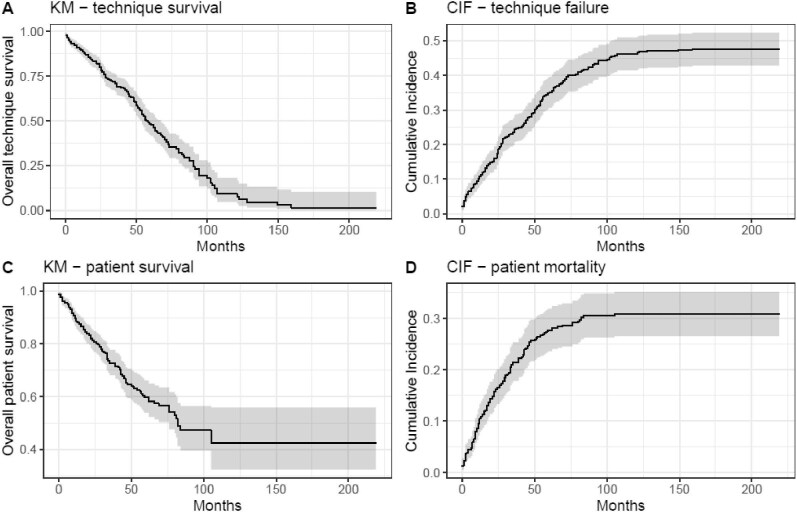
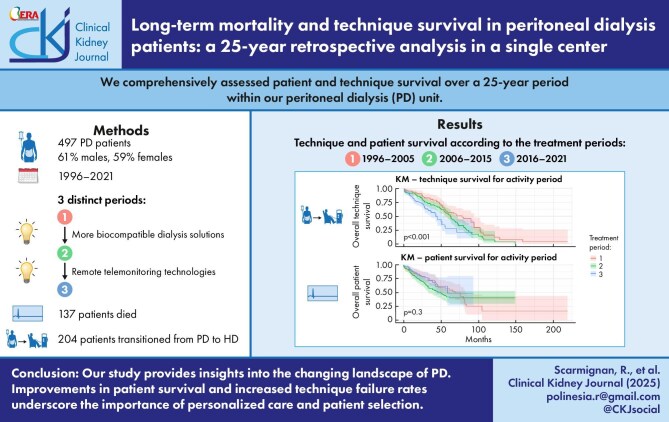
Background: We comprehensively assessed patient survival and the duration of peritoneal dialysis (PD) treatment over a 25-year period within our PD unit.
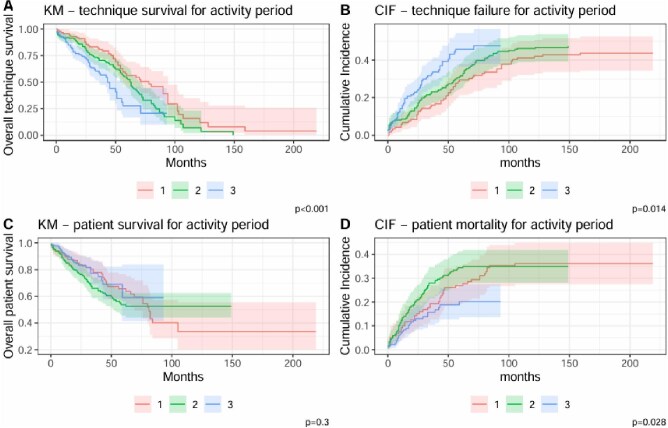
Methods: We retrospectively evaluated 497 PD patients who initiated PD between 1996 and 2021. The cohort was divided into three distinct periods based on pivotal events, such as the introduction of more biocompatible dialysis solutions and the initiation of remote monitoring technologies. Kaplan-Meier survival assessments, Cox proportional hazards model and Gray subdistribution hazard model were employed to evaluate patient survival and PD-to-hemodialysis (HD) transfer.
Results: The use of PD as the initial treatment increased significantly over the years. Mean age was 63.5 ± 15.7 years; 61% were male, and 61% had three or more comorbidities including hypertension (81%), dyslipidemia (66%), cardiovascular disease (56%) and diabetes (16%). The five-year mortality rate was 40%. Risk factors for mortality included continuous ambulatory peritoneal dialysis (CAPD) [hazard ratio (HR) = 2.63, 95% confidence interval (CI) 1.76-3.93; P < .001], older age (HR = 2.96, 95% CI 1.98-4.43; P < .001), cardiovascular disease (HR = 1.96, 95% CI 1.31-2.95; P = .001) and the use of renin-angiotensin-aldosterone system inhibitors (RAASi) (HR = 1.81, 95% CI 1.22-2.70; P = .004). At 5 years, 48% of patients remained on PD. In the Cox model, risk factors for PD-to-HD transfer included CAPD (HR = 1.62, 95% CI 1.21-2.16; P = .001). RAASi use (HR = 0.66, 95% CI 0.46-0.94; P = .02) and female sex (HR = 0.70, 95% CI 0.51-0.96; P = .03) were associated with longer PD duration.
Conclusions: The study provides insights into the changing landscape of PD. Advances in PD solutions and remote monitoring have contributed to changes in PD outcomes and its increased adoption over the years. Given the observational nature of the study, caution is warranted in interpreting the association of both CAPD and RAASi with mortality.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


