{"title":"静脉铁治疗对血液透析患者死亡率和心血管事件的影响:一项荟萃分析","authors":"Yan Chen, Dian Zhao, Chong Huang, Yanxia Chen, Weiping Tu, Chengyun Xu","doi":"10.17305/bb.2025.12652","DOIUrl":null,"url":null,"abstract":"<p><p>Intravenous (IV) iron is widely utilized to manage anemia in patients undergoing maintenance hemodialysis; however, its long-term safety remains uncertain. This meta-analysis aimed to evaluate the impact of IV iron on all-cause mortality and major adverse cardiovascular events (MACEs) within this population. We conducted a systematic search of PubMed, Embase, Cochrane Library, Web of Science, Wanfang, and CNKI up to March 2025 for randomized controlled trials (RCTs) that compared IV iron with placebo/usual care, oral iron, or varying doses of IV iron in adult hemodialysis patients. The primary outcomes assessed were all-cause mortality and MACEs. Data were synthesized using a random-effects model, and the quality of evidence was evaluated employing the GRADE approach. A total of fifteen RCTs involving 4,257 patients were included in the analysis. Compared to placebo/usual care, IV iron did not significantly affect all-cause mortality (OR: 1.36; 95% CI: 0.60-3.09) or MACEs (OR: 0.81; 95% CI: 0.43-1.55), with a moderate level of evidence. Furthermore, IV iron demonstrated no significant differences in mortality (OR: 0.58; 95% CI: 0.18-1.90) or MACEs (OR: 2.47; 95% CI: 0.37-16.34) when compared to oral iron, although the quality of evidence in this comparison was very low. High-dose IV iron was associated with a reduced mortality rate compared to low-dose IV iron (OR: 0.81; 95% CI: 0.67-0.97), though this result was influenced by a single large study. In conclusion, IV iron does not appear to increase mortality or MACEs relative to placebo or oral iron. While high-dose IV iron may decrease mortality, the evidence remains limited, indicating a need for further research.</p>","PeriodicalId":72398,"journal":{"name":"Biomolecules & biomedicine","volume":" ","pages":"65-78"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499556/pdf/","citationCount":"0","resultStr":"{\"title\":\"Influence of intravenous iron therapy on mortality and cardiovascular events of patients on hemodialysis: A meta-analysis.\",\"authors\":\"Yan Chen, Dian Zhao, Chong Huang, Yanxia Chen, Weiping Tu, Chengyun Xu\",\"doi\":\"10.17305/bb.2025.12652\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Intravenous (IV) iron is widely utilized to manage anemia in patients undergoing maintenance hemodialysis; however, its long-term safety remains uncertain. This meta-analysis aimed to evaluate the impact of IV iron on all-cause mortality and major adverse cardiovascular events (MACEs) within this population. We conducted a systematic search of PubMed, Embase, Cochrane Library, Web of Science, Wanfang, and CNKI up to March 2025 for randomized controlled trials (RCTs) that compared IV iron with placebo/usual care, oral iron, or varying doses of IV iron in adult hemodialysis patients. The primary outcomes assessed were all-cause mortality and MACEs. Data were synthesized using a random-effects model, and the quality of evidence was evaluated employing the GRADE approach. A total of fifteen RCTs involving 4,257 patients were included in the analysis. Compared to placebo/usual care, IV iron did not significantly affect all-cause mortality (OR: 1.36; 95% CI: 0.60-3.09) or MACEs (OR: 0.81; 95% CI: 0.43-1.55), with a moderate level of evidence. Furthermore, IV iron demonstrated no significant differences in mortality (OR: 0.58; 95% CI: 0.18-1.90) or MACEs (OR: 2.47; 95% CI: 0.37-16.34) when compared to oral iron, although the quality of evidence in this comparison was very low. High-dose IV iron was associated with a reduced mortality rate compared to low-dose IV iron (OR: 0.81; 95% CI: 0.67-0.97), though this result was influenced by a single large study. In conclusion, IV iron does not appear to increase mortality or MACEs relative to placebo or oral iron. While high-dose IV iron may decrease mortality, the evidence remains limited, indicating a need for further research.</p>\",\"PeriodicalId\":72398,\"journal\":{\"name\":\"Biomolecules & biomedicine\",\"volume\":\" \",\"pages\":\"65-78\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499556/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomolecules & biomedicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17305/bb.2025.12652\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomolecules & biomedicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17305/bb.2025.12652","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Influence of intravenous iron therapy on mortality and cardiovascular events of patients on hemodialysis: A meta-analysis.
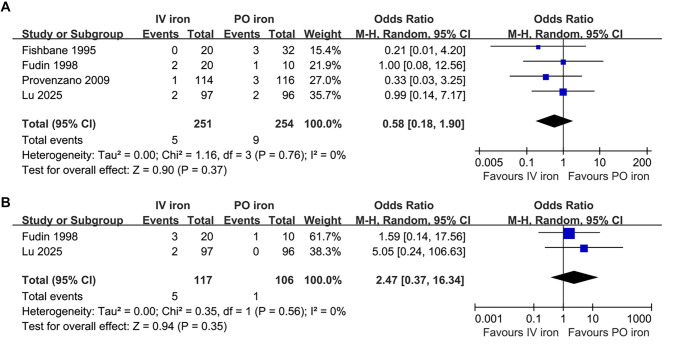
Intravenous (IV) iron is widely utilized to manage anemia in patients undergoing maintenance hemodialysis; however, its long-term safety remains uncertain. This meta-analysis aimed to evaluate the impact of IV iron on all-cause mortality and major adverse cardiovascular events (MACEs) within this population. We conducted a systematic search of PubMed, Embase, Cochrane Library, Web of Science, Wanfang, and CNKI up to March 2025 for randomized controlled trials (RCTs) that compared IV iron with placebo/usual care, oral iron, or varying doses of IV iron in adult hemodialysis patients. The primary outcomes assessed were all-cause mortality and MACEs. Data were synthesized using a random-effects model, and the quality of evidence was evaluated employing the GRADE approach. A total of fifteen RCTs involving 4,257 patients were included in the analysis. Compared to placebo/usual care, IV iron did not significantly affect all-cause mortality (OR: 1.36; 95% CI: 0.60-3.09) or MACEs (OR: 0.81; 95% CI: 0.43-1.55), with a moderate level of evidence. Furthermore, IV iron demonstrated no significant differences in mortality (OR: 0.58; 95% CI: 0.18-1.90) or MACEs (OR: 2.47; 95% CI: 0.37-16.34) when compared to oral iron, although the quality of evidence in this comparison was very low. High-dose IV iron was associated with a reduced mortality rate compared to low-dose IV iron (OR: 0.81; 95% CI: 0.67-0.97), though this result was influenced by a single large study. In conclusion, IV iron does not appear to increase mortality or MACEs relative to placebo or oral iron. While high-dose IV iron may decrease mortality, the evidence remains limited, indicating a need for further research.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


