{"title":"联合动脉重建和手术远端静脉动脉化治疗血栓闭塞性脉管炎保肢1例报告。","authors":"Yuri Yoshida, Shinsuke Kikuchi, Daichi Mizushima, Hirofumi Jinno, Hiroya Moriyama, Takayuki Uramoto, Kazuki Takahashi, Tsutomu Doita, Keisuke Kamada, Seima Ohira, Daiki Uchida, Naoya Kuriyama, Nobuyoshi Azuma","doi":"10.70352/scrj.cr.25-0342","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Thromboangiitis obliterans (TAO) has become increasingly uncommon in Japan due to declining smoking prevalence. However, in advanced cases with severely compromised distal vasculature, achieving durable limb salvage remains a formidable surgical challenge.</p><p><strong>Case presentation: </strong>A 51-year-old man with a 12-year history of TAO presented with rest pain and a necrotic ulcer on the 2nd toe. He had recently ceased smoking after a 31-year history. Imaging demonstrated complete occlusion of the popliteal and tibial arteries, with foot perfusion reliant on corkscrew collaterals. The ankle-brachial index was 0.43, and skin perfusion pressure (SPP) was critically low. A severely diseased plantar artery was identified as a potential distal target. Given the high risk of graft failure, a hybrid strategy combining <i>in situ</i> bypass and surgical distal venous arterialization (DVA) was preoperatively planned. To mitigate perioperative vasospasm, a lumbar sympathetic block was administered 1 week prior to surgery. An <i>in situ</i> bypass using the ipsilateral great saphenous vein was constructed from the superficial femoral artery to the plantar artery. DVA was established via retrograde puncture of the plantar vein, balloon angioplasty for valve sites, and end-to-side anastomosis to the bypass graft. Early duplex ultrasonography revealed anastomotic stenosis at the DVA site as well as stenosis at valve sites, both of which were successfully managed with a single endovascular procedure. The toe stump healed completely within 3 months. The graft remained patent for 2 years, and SPP was preserved even after graft occlusion. Notably, graft failure coincided with DVA occlusion, suggesting its critical role in maintaining flow. At 42 months postoperatively, the patient remained ulcer-free with favorable perfusion, pain-free ambulation, and full return to work.</p><p><strong>Conclusions: </strong>Preoperatively planned surgical DVA, in conjunction with sympathetic modulation and timely postoperative intervention, may offer a durable limb salvage strategy in advanced TAO with limited distal targets.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12313424/pdf/","citationCount":"0","resultStr":"{\"title\":\"Combined Arterial Reconstruction and Surgical Distal Venous Arterialization for Limb Salvage in Thromboangiitis Obliterans: A Case Report.\",\"authors\":\"Yuri Yoshida, Shinsuke Kikuchi, Daichi Mizushima, Hirofumi Jinno, Hiroya Moriyama, Takayuki Uramoto, Kazuki Takahashi, Tsutomu Doita, Keisuke Kamada, Seima Ohira, Daiki Uchida, Naoya Kuriyama, Nobuyoshi Azuma\",\"doi\":\"10.70352/scrj.cr.25-0342\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Thromboangiitis obliterans (TAO) has become increasingly uncommon in Japan due to declining smoking prevalence. However, in advanced cases with severely compromised distal vasculature, achieving durable limb salvage remains a formidable surgical challenge.</p><p><strong>Case presentation: </strong>A 51-year-old man with a 12-year history of TAO presented with rest pain and a necrotic ulcer on the 2nd toe. He had recently ceased smoking after a 31-year history. Imaging demonstrated complete occlusion of the popliteal and tibial arteries, with foot perfusion reliant on corkscrew collaterals. The ankle-brachial index was 0.43, and skin perfusion pressure (SPP) was critically low. A severely diseased plantar artery was identified as a potential distal target. Given the high risk of graft failure, a hybrid strategy combining <i>in situ</i> bypass and surgical distal venous arterialization (DVA) was preoperatively planned. To mitigate perioperative vasospasm, a lumbar sympathetic block was administered 1 week prior to surgery. An <i>in situ</i> bypass using the ipsilateral great saphenous vein was constructed from the superficial femoral artery to the plantar artery. DVA was established via retrograde puncture of the plantar vein, balloon angioplasty for valve sites, and end-to-side anastomosis to the bypass graft. Early duplex ultrasonography revealed anastomotic stenosis at the DVA site as well as stenosis at valve sites, both of which were successfully managed with a single endovascular procedure. The toe stump healed completely within 3 months. The graft remained patent for 2 years, and SPP was preserved even after graft occlusion. Notably, graft failure coincided with DVA occlusion, suggesting its critical role in maintaining flow. At 42 months postoperatively, the patient remained ulcer-free with favorable perfusion, pain-free ambulation, and full return to work.</p><p><strong>Conclusions: </strong>Preoperatively planned surgical DVA, in conjunction with sympathetic modulation and timely postoperative intervention, may offer a durable limb salvage strategy in advanced TAO with limited distal targets.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12313424/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0342\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0342","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Combined Arterial Reconstruction and Surgical Distal Venous Arterialization for Limb Salvage in Thromboangiitis Obliterans: A Case Report.
Introduction: Thromboangiitis obliterans (TAO) has become increasingly uncommon in Japan due to declining smoking prevalence. However, in advanced cases with severely compromised distal vasculature, achieving durable limb salvage remains a formidable surgical challenge.
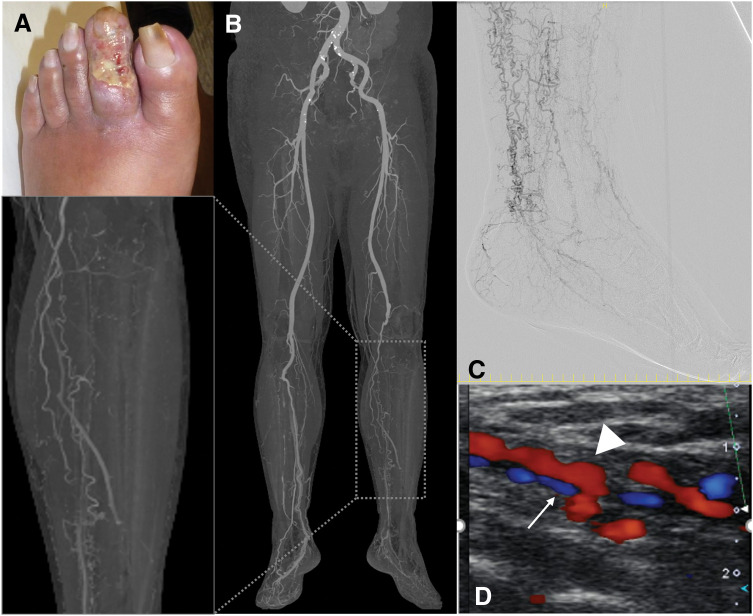
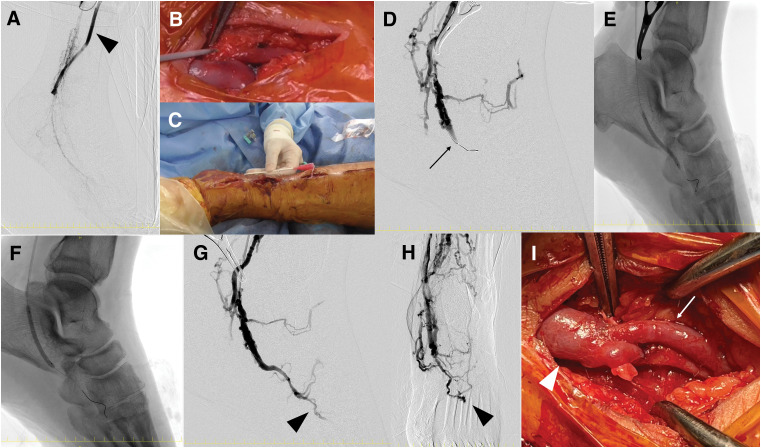
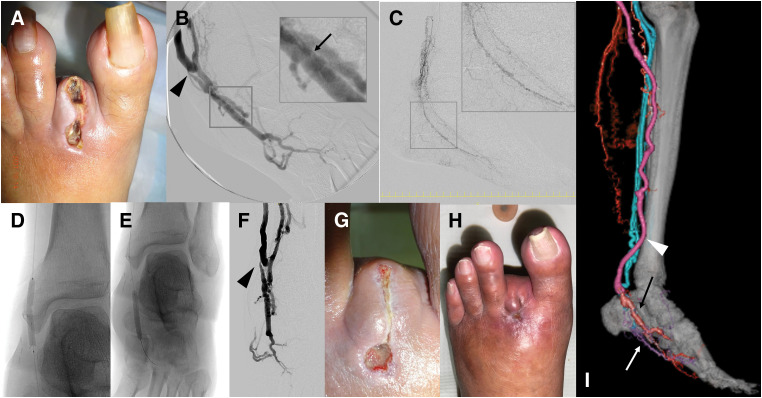
Case presentation: A 51-year-old man with a 12-year history of TAO presented with rest pain and a necrotic ulcer on the 2nd toe. He had recently ceased smoking after a 31-year history. Imaging demonstrated complete occlusion of the popliteal and tibial arteries, with foot perfusion reliant on corkscrew collaterals. The ankle-brachial index was 0.43, and skin perfusion pressure (SPP) was critically low. A severely diseased plantar artery was identified as a potential distal target. Given the high risk of graft failure, a hybrid strategy combining in situ bypass and surgical distal venous arterialization (DVA) was preoperatively planned. To mitigate perioperative vasospasm, a lumbar sympathetic block was administered 1 week prior to surgery. An in situ bypass using the ipsilateral great saphenous vein was constructed from the superficial femoral artery to the plantar artery. DVA was established via retrograde puncture of the plantar vein, balloon angioplasty for valve sites, and end-to-side anastomosis to the bypass graft. Early duplex ultrasonography revealed anastomotic stenosis at the DVA site as well as stenosis at valve sites, both of which were successfully managed with a single endovascular procedure. The toe stump healed completely within 3 months. The graft remained patent for 2 years, and SPP was preserved even after graft occlusion. Notably, graft failure coincided with DVA occlusion, suggesting its critical role in maintaining flow. At 42 months postoperatively, the patient remained ulcer-free with favorable perfusion, pain-free ambulation, and full return to work.
Conclusions: Preoperatively planned surgical DVA, in conjunction with sympathetic modulation and timely postoperative intervention, may offer a durable limb salvage strategy in advanced TAO with limited distal targets.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


