Sebastian Mussnig, Simon Krenn, Max Waller, Michael Schmiedecker, Amelie Kurnikowski, Janosch Niknam Saeidi, Luis Naar, Christopher C Mayer, David Keane, Daniel Schneditz, Manfred Hecking, Leszek Pstras
{"title":"液体超载、血容量和血管再充盈的纵向模式:维持性血液透析患者的前瞻性研究","authors":"Sebastian Mussnig, Simon Krenn, Max Waller, Michael Schmiedecker, Amelie Kurnikowski, Janosch Niknam Saeidi, Luis Naar, Christopher C Mayer, David Keane, Daniel Schneditz, Manfred Hecking, Leszek Pstras","doi":"10.1093/ckj/sfaf199","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients on maintenance hemodialysis accumulate excess fluid between treatments. Intradialytic removal of fluid via ultrafiltration is partly compensated by vascular refilling from the interstitial space. Associations between whole-body fluid status and blood volume were previously investigated on the population level. The aim of this observational cohort study was to assess longitudinal changes in fluid compartment volumes on an intra-patient level.</p><p><strong>Methodology: </strong>Pre-dialysis bioimpedance spectroscopy measurements and absolute blood volume estimations were conducted in maintenance hemodialysis patients during 14 consecutive dialysis treatments over 5 weeks. Blood volume was determined using the dialysate bolus method. Longitudinal changes were evaluated using linear mixed models. Correlations were analyzed with repeated measures correlation coefficients ([Formula: see text]).</p><p><strong>Results: </strong>Twenty-five patients were included in the final analysis [88% male, median (quartile 1, quartile 3) age and dialysis vintage of 66.0 years (48.0, 74.0) and 23.5 months (13.5, 34.5), respectively]. Pre-dialysis fluid overload significantly decreased from the first to the third treatment within the week (<i>β</i> = -0.38, <i>P</i> < .01) with no significant within-week changes in euvolemic body mass (<i>β</i>= -0.04, <i>P</i> = .78) or absolute blood volume at treatment start (<i>β</i> = -0.06, <i>P</i> = .65). Fluid overload did not correlate with absolute ([Formula: see text] = 0.10, <i>P</i> = .65) or specific blood volume ([Formula: see text]=0.06, <i>P</i> = .78) at treatment start on an intra-patient level, but correlated moderately with refilling volume ([Formula: see text] = 0.46, <i>P</i> < .01).</p><p><strong>Conclusions: </strong>The observed lack of intra-patient correlations between pre-dialysis fluid overload and blood volume suggests that excess fluid may not necessarily accumulate proportionally in the interstitial and intravascular space, thus challenging previous assumptions regarding within-week changes in fluid compartments.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 8","pages":"sfaf199"},"PeriodicalIF":4.6000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314271/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal patterns of fluid overload, blood volume and vascular refilling: a prospective study in patients on maintenance hemodialysis.\",\"authors\":\"Sebastian Mussnig, Simon Krenn, Max Waller, Michael Schmiedecker, Amelie Kurnikowski, Janosch Niknam Saeidi, Luis Naar, Christopher C Mayer, David Keane, Daniel Schneditz, Manfred Hecking, Leszek Pstras\",\"doi\":\"10.1093/ckj/sfaf199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Patients on maintenance hemodialysis accumulate excess fluid between treatments. Intradialytic removal of fluid via ultrafiltration is partly compensated by vascular refilling from the interstitial space. Associations between whole-body fluid status and blood volume were previously investigated on the population level. The aim of this observational cohort study was to assess longitudinal changes in fluid compartment volumes on an intra-patient level.</p><p><strong>Methodology: </strong>Pre-dialysis bioimpedance spectroscopy measurements and absolute blood volume estimations were conducted in maintenance hemodialysis patients during 14 consecutive dialysis treatments over 5 weeks. Blood volume was determined using the dialysate bolus method. Longitudinal changes were evaluated using linear mixed models. Correlations were analyzed with repeated measures correlation coefficients ([Formula: see text]).</p><p><strong>Results: </strong>Twenty-five patients were included in the final analysis [88% male, median (quartile 1, quartile 3) age and dialysis vintage of 66.0 years (48.0, 74.0) and 23.5 months (13.5, 34.5), respectively]. Pre-dialysis fluid overload significantly decreased from the first to the third treatment within the week (<i>β</i> = -0.38, <i>P</i> < .01) with no significant within-week changes in euvolemic body mass (<i>β</i>= -0.04, <i>P</i> = .78) or absolute blood volume at treatment start (<i>β</i> = -0.06, <i>P</i> = .65). Fluid overload did not correlate with absolute ([Formula: see text] = 0.10, <i>P</i> = .65) or specific blood volume ([Formula: see text]=0.06, <i>P</i> = .78) at treatment start on an intra-patient level, but correlated moderately with refilling volume ([Formula: see text] = 0.46, <i>P</i> < .01).</p><p><strong>Conclusions: </strong>The observed lack of intra-patient correlations between pre-dialysis fluid overload and blood volume suggests that excess fluid may not necessarily accumulate proportionally in the interstitial and intravascular space, thus challenging previous assumptions regarding within-week changes in fluid compartments.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 8\",\"pages\":\"sfaf199\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314271/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf199\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf199","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
导读:维持性血液透析患者在两次治疗之间会积累过多的液体。通过超滤去除的液体部分由间隙的血管再填充来补偿。全体液状态和血容量之间的关系以前在人群水平上进行过调查。本观察性队列研究的目的是在患者水平上评估液室容积的纵向变化。方法:对维持性血液透析患者进行透析前生物阻抗谱测量和绝对血容量估计,连续透析14次,持续5周。采用透析液丸法测定血容量。使用线性混合模型评估纵向变化。用重复测量相关系数分析相关性(公式:见文)。结果:最终纳入25例患者[88%为男性,中位年龄(四分位数1,四分位数3)为66.0岁(48.0,74.0),透析时间为23.5个月(13.5,34.5)]。透析前液体负荷在一周内从第一次治疗到第三次治疗显著降低(β = -0.38, P β= -0.04, P = 0.78)或治疗开始时绝对血容量显著降低(β = -0.06, P = 0.65)。在治疗开始时,液体过载与患者内部的绝对血容量([公式:见文]= 0.10,P = 0.65)或特定血容量([公式:见文]=0.06,P = 0.78)无关,但与再灌注量([公式:见文]= 0.46,P)中度相关。观察到的透析前液体超载与血容量之间缺乏患者内部相关性表明,过量的液体可能不一定成比例地积聚在间质和血管内空间,从而挑战了先前关于周内液体室变化的假设。
Longitudinal patterns of fluid overload, blood volume and vascular refilling: a prospective study in patients on maintenance hemodialysis.
Introduction: Patients on maintenance hemodialysis accumulate excess fluid between treatments. Intradialytic removal of fluid via ultrafiltration is partly compensated by vascular refilling from the interstitial space. Associations between whole-body fluid status and blood volume were previously investigated on the population level. The aim of this observational cohort study was to assess longitudinal changes in fluid compartment volumes on an intra-patient level.
Methodology: Pre-dialysis bioimpedance spectroscopy measurements and absolute blood volume estimations were conducted in maintenance hemodialysis patients during 14 consecutive dialysis treatments over 5 weeks. Blood volume was determined using the dialysate bolus method. Longitudinal changes were evaluated using linear mixed models. Correlations were analyzed with repeated measures correlation coefficients ([Formula: see text]).
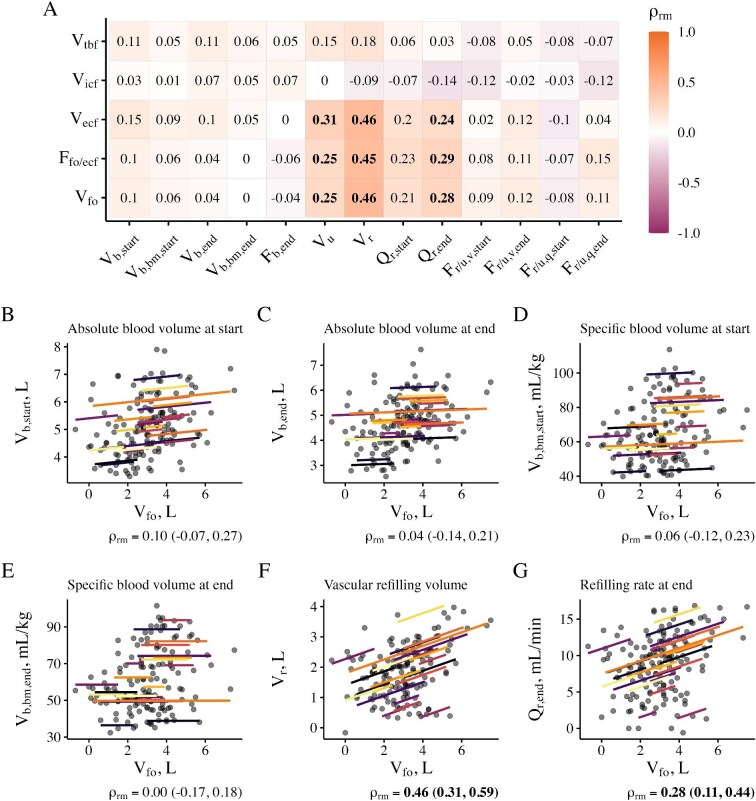
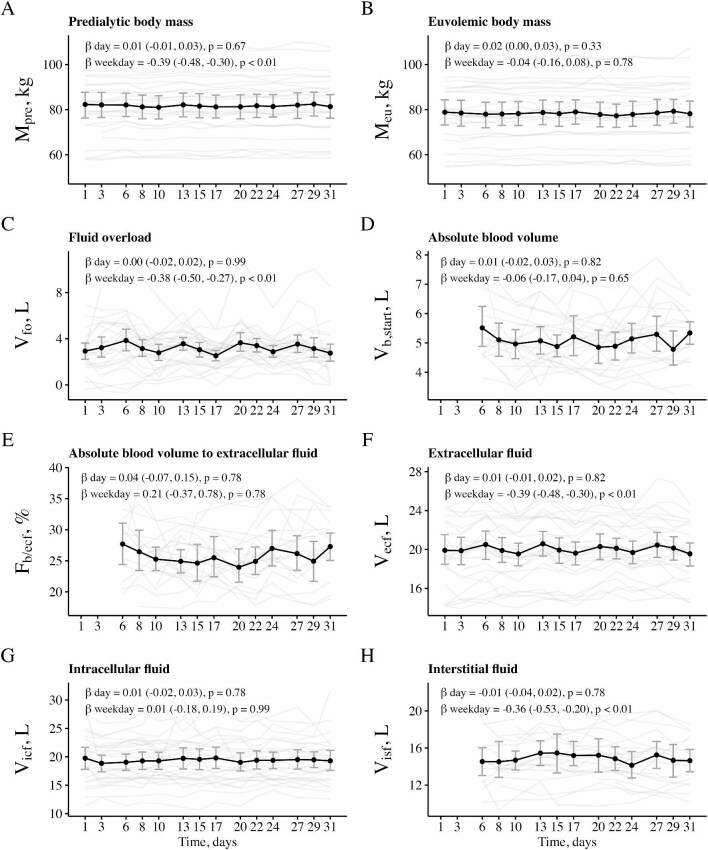
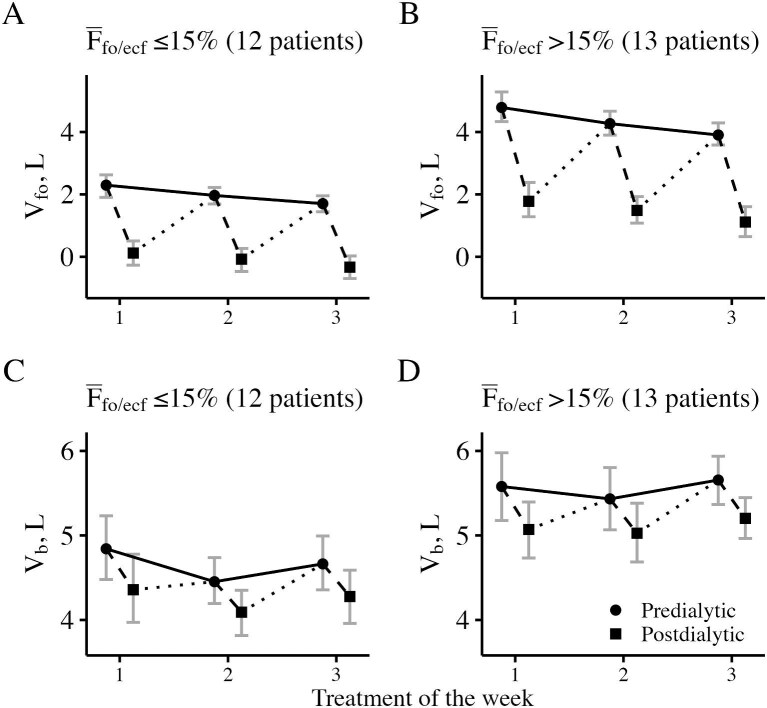
Results: Twenty-five patients were included in the final analysis [88% male, median (quartile 1, quartile 3) age and dialysis vintage of 66.0 years (48.0, 74.0) and 23.5 months (13.5, 34.5), respectively]. Pre-dialysis fluid overload significantly decreased from the first to the third treatment within the week (β = -0.38, P < .01) with no significant within-week changes in euvolemic body mass (β= -0.04, P = .78) or absolute blood volume at treatment start (β = -0.06, P = .65). Fluid overload did not correlate with absolute ([Formula: see text] = 0.10, P = .65) or specific blood volume ([Formula: see text]=0.06, P = .78) at treatment start on an intra-patient level, but correlated moderately with refilling volume ([Formula: see text] = 0.46, P < .01).
Conclusions: The observed lack of intra-patient correlations between pre-dialysis fluid overload and blood volume suggests that excess fluid may not necessarily accumulate proportionally in the interstitial and intravascular space, thus challenging previous assumptions regarding within-week changes in fluid compartments.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


